Practice Essentials
Schatzki rings are fixed anatomic mucosal ring structures in the distal esophagus. They are distinct from lower esophageal muscular rings (A rings), which are transient, smooth, circumferential indentations in the esophagus. Lower esophageal rings were described first by Templeton in 1944. The vast majority of patients with lower esophageal rings are asymptomatic. In fact, lower esophageal rings are found during 6-14% of all routine upper gastrointestinal barium examinations. Lower esophageal rings that cause symptoms (true Schatzki rings) occur in only 0.5% of patients undergoing these examinations. Schatzki rings are a common cause of intermittent dysphagia. The association of intermittent dysphagia with lower esophageal rings was reported by Ingelfinger and Kramer and also by Schatzki and Gary in 1953. [1, 2, 3, 4, 5, 6]
Imaging modalities
Barium esophagography is the preferred method of detection of Schatzki rings. Single-contrast esophagography performed with the patient drinking in the prone position is more sensitive in detecting lower esophageal mucosal rings than is erect double-contrast imaging of the esophagus. [7]
Upper gastrointestinal endoscopy is commonly used for the evaluation of dysphagia. Upper endoscopy may not be as sensitive as barium esophagography in detecting lower esophageal rings. [8] In one study, endoscopy failed to depict more than one third of radiologically demonstrated lower esophageal rings, half of which had caused symptoms and dysphagia.
Esophageal rings may be missed during barium esophagography if distention of the distal esophagus is inadequate; therefore, adequate distention of the esophagus during barium esophagography is imperative. This distention is best achieved by using a single-contrast technique in the prone or right or left anterior oblique position with large boluses of barium. A modified Valsalva maneuver also may help in demonstrating the ring by distending the associated hiatal hernia.
The goal of treatment is to reduce the diameter of the ring to allow passage through the esophagus. Methods include dilation or biopsies of the ring with a biopsy forceps. [1]
(See the images below.)
 Schatzki ring on an erect, double-contrast barium esophagogram. Image demonstrates a thin, ringlike narrowing (arrows) in the lower esophagus just above a hiatal hernia.
Schatzki ring on an erect, double-contrast barium esophagogram. Image demonstrates a thin, ringlike narrowing (arrows) in the lower esophagus just above a hiatal hernia.
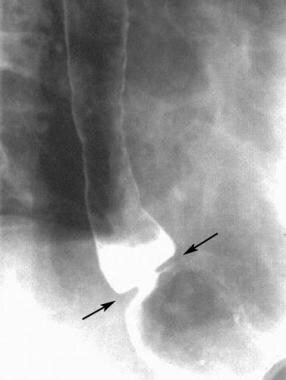
 Schatzki ring. Prone, single-contrast barium esophagogram demonstrating a thin, ringlike narrowing (arrows) in the lower esophagus just above a hiatal hernia. This view is most sensitive for detecting lower esophageal rings, provided adequate esophageal distention is achieved.
Schatzki ring. Prone, single-contrast barium esophagogram demonstrating a thin, ringlike narrowing (arrows) in the lower esophagus just above a hiatal hernia. This view is most sensitive for detecting lower esophageal rings, provided adequate esophageal distention is achieved.
Pathophysiology
The pathophysiology of Schatzki ring is not fully known. Various hypotheses include congenital origin, arising from a pleat of redundant mucosa, or as a result of gastroesophageal reflux or esophagitis. [1, 9]
Some investigators have demonstrated that Schatzki rings become narrowed during serial radiographic examinations and that they transform into actual peptic strictures. Even so, endoscopic biopsy and 24-hour esophageal pH monitoring have failed to show any symptoms or signs of gastroesophageal reflux or reflux esophagitis in more than one third of patients with Schatzki rings.
Schatzki ring is a common cause of intermittent dysphagia. In fact, in a large endoscopic series, it was the fourth most common endoscopic finding in endoscopic evaluation of dysphagia after esophageal stricture, normal endoscopy, and esophagitis/ulcer. [4] Although several studies have considered an association between Schatzki rings and eosinophilic esophagitis, a systematic review and meta-analysis could not find a significant relationship between the 2 disorders. [10]
Morbidity
The primary morbidity associated with lower esophageal rings is dysphagia, but many patients remain asymptomatic. Schatzki ring is a common cause of dysphagia. Typically, the dysphagia is intermittent or short-lived. Food may become stuck in the esophagus but can be forced down by drinking liquids or may be regurgitated. The dysphagia may not recur for months or years. Patients may have associated symptoms of gastroesophageal reflux.
The differential diagnosis includes the following:
-
Focal esophageal carcinoma
Radiography
On barium esophagography, lower esophageal mucosal rings are manifested by a thin circumferential constriction at the gastroesophageal junction. These rings almost always are associated with a sliding hiatal hernia. The ring itself has smooth, symmetric margins and is only 2-4 mm in height. The finding of a fixed, smooth, narrow, circumferential ring at the esophagogastric junction in a patient with dysphagia is virtually diagnostic of a Schatzki ring. [11, 12, 13, 14]
(See the image below).
Schatzki ring on an erect, double-contrast barium esophagogram. Image demonstrates a thin, ringlike narrowing (arrows) in the lower esophagus just above a hiatal hernia.
As with all esophageal rings and strictures, the lumen of the esophagus has to be dilated beyond the caliber of the ring if the ring is to be visualized; therefore, adequate distention of the distal esophagus is of paramount importance and is achieved best by using single-contrast, prone examinations.
(See the image below.)
Schatzki ring. Prone, single-contrast barium esophagogram demonstrating a thin, ringlike narrowing (arrows) in the lower esophagus just above a hiatal hernia. This view is most sensitive for detecting lower esophageal rings, provided adequate esophageal distention is achieved.
A barium pill of known diameter (eg, 12 mm) may be used at the end of the examination to determine the functional luminal caliber of the ring. Most symptomatic rings (true Schatzki rings) are 13 mm or less in caliber.
False positive/negatives
In addition to Schatzki rings, other causes of distal esophageal narrowing are a ringlike peptic stricture, a lower esophageal muscular ring (A ring), focal esophageal cancer, and an esophageal web.
Focal annular peptic strictures are usually asymmetric, and they often have a vertical thickness greater than 5 mm. Lower esophageal muscular rings, also termed contractile rings or A rings, are a normal area of contraction in the distal esophagus located a few centimeters above the gastroesophageal junction. These should not be confused with Schatzki rings.
In contrast to Schatzki rings, which are fixed anatomic mucosal structures, lower esophageal muscular rings are transient, smooth, thick, circumferential indentations in the esophagus. If observed long enough during the course of the examination, these muscular rings will relax and disappear.
A patient may have both a mucosal ring at the gastroesophageal junction and a muscular ring a few centimeters more proximal.
A focal carcinoma of the lower esophagus should not be confused with a mucosal ring. In contrast to Schatzki rings, esophageal cancers have an irregular contour; they are asymmetric; and they have shelflike borders within the narrowed segment. These features help distinguish them from true mucosal rings.
Uncommonly, esophageal webs can be circumferential and resemble a mucosal ring, but they are most commonly found in the cervical esophagus. Rarely, esophageal webs can be found in the distal esophagus, but these webs are located above the gastroesophageal junction; therefore, they can be differentiated from lower esophageal mucosal rings. More often than not, esophageal webs do not produce a complete circumferential ring and appear as only a thin indentation on one side of the esophagus.
-
Schatzki ring on an erect, double-contrast barium esophagogram. Image demonstrates a thin, ringlike narrowing (arrows) in the lower esophagus just above a hiatal hernia.
-
Schatzki ring. Prone, single-contrast barium esophagogram demonstrating a thin, ringlike narrowing (arrows) in the lower esophagus just above a hiatal hernia. This view is most sensitive for detecting lower esophageal rings, provided adequate esophageal distention is achieved.




