Practice Essentials
Prune belly syndrome (PBS), also known as Eagle-Barrett syndrome, is characterized by a triad of symptoms consisting of deficiency of the abdominal muscles, malformations of the urinary tract, and bilateral cryptorchidism. Perinatal mortality rates are high, ranging from 10 to 25%, with early death primarily attributed to the degree of prematurity and pulmonary hypoplasia. PBS typically occurs in boys, with a thin or lax abdominal wall, but laxity is variable in severity. The prostatic urethra is long and dilated as a result of prostatic hypoplasia. Some patients have a urachal diverticulum; a large, vertically oriented, thick-walled bladder; and tortuous and dilated ureters. Varying amounts of hydronephrosis and varying degrees of renal dysplasia are seen. [1, 2, 3, 4, 5]
The amniotic fluid volume may be normal or decreased in neonates with prune belly syndrome. The presence of oligohydramnios may account for some of the accompanying findings of the extremities. [6, 7, 8]
The etiology of prune belly syndrome is not fully understood. The thinness of the abdominal wall has been attributed to hydronephrosis. The distended urinary system is thought to interfere with the normal descent of the testes. However, some patients with severe hydronephrosis do not have the same disorder of the abdominal wall. Cryptorchidism usually is not seen in patients with distended bladders of other etiology. [9, 10]
Prune belly syndrome is a rare anomaly, with an incidence of 3.8 per 100,000 live male births in the United States. Females represent less than 5% of all cases, and they present with abdominal wall deficiency and a dilated, dysmorphic urinary tract. The genetic origins remain unclear. [2, 11, 12, 13, 14]
(See the images below.)
 The abdomen of an infant with prune belly syndrome shows marked distention of the abdomen and bulging flanks secondary to a large urinary system and the absence of abdominal wall musculature.
The abdomen of an infant with prune belly syndrome shows marked distention of the abdomen and bulging flanks secondary to a large urinary system and the absence of abdominal wall musculature.
 Ultrasound examination of the kidneys shows bilateral hyperechoic kidneys with poor development of the calyces and dilated tortuous ureters.
Ultrasound examination of the kidneys shows bilateral hyperechoic kidneys with poor development of the calyces and dilated tortuous ureters.
 On CT, the ureter in this patient with prune belly syndrome fills the entire abdomen.
On CT, the ureter in this patient with prune belly syndrome fills the entire abdomen.
Preferred examination
Prenatal ultrasonography can usually diagnose prune belly syndrome. [2] Features can be identified in the first trimester, but diagnosis is more common in the second trimester, when the classic findings of hydroureteronephrosis, megacystis, irregular abdominal wall circumference, and oligohydramnios can be accurately identified. [15, 2]
To confirm prune belly syndrome, radiography is used to evaluate the abdomen and chest initially. For urinary tract evaluation, renal US and voiding cystourethrography are performed. [16, 5] For fragile neonates and for infants with severe reflux and retention, these simple diagnostic studies may be much more threatening than they are for the normal baby. The use of prophylactic antibiotics and the need to act upon the study results should be weighed before proceeding indiscriminately.
Some diagnosticians assess renal function by performing a technetium-99m (99mTc) dimethylsuccinic acid (DMSA) renal scan. DMSA is a cortical agent; DMSA renal scans provide information about both the appearance and the function of the kidneys.
Radiography
Radiographic findings in prune belly syndrome are as follows:
-
Chest: Hypoplastic lungs, flaring of the lower ribs secondary to the distended abdomen is seen (see the image below).
 Note the small lung volumes and constriction of the upper thorax. Flaring of the lower ribs secondary to distention of the abdomen is seen. Infants with prune belly syndrome may develop severe respiratory distress secondary to the thoracic limitation.
Note the small lung volumes and constriction of the upper thorax. Flaring of the lower ribs secondary to distention of the abdomen is seen. Infants with prune belly syndrome may develop severe respiratory distress secondary to the thoracic limitation.
-
Abdomen: Diffusely distended flanks are seen. Masslike areas in the abdomen represent a hydronephrotic urinary tract (see the image below).
 The abdomen of an infant with prune belly syndrome shows marked distention of the abdomen and bulging flanks secondary to a large urinary system and the absence of abdominal wall musculature.
The abdomen of an infant with prune belly syndrome shows marked distention of the abdomen and bulging flanks secondary to a large urinary system and the absence of abdominal wall musculature.
-
Kidneys: Dilated, clubbed, and dysplastic calyces are seen. Renal parenchyma often is hyperechoic on US, which shows poor development and differentiation of the calyces. Often, small cysts are seen in the subcapsular cortex.
-
Ureters: Ureters are markedly dilated and tortuous, with involvement more severe distally. Usually, refluxing ureters are seen (see the image below).
 Infants with prune belly syndrome show early and marked bilateral vesicoureteral reflux. Significantly more dilatation of the lower ureters exists.
Infants with prune belly syndrome show early and marked bilateral vesicoureteral reflux. Significantly more dilatation of the lower ureters exists.
-
Bladder: The bladder is vertical and trabeculated, with a urachal remnant at the dome. The base of the bladder is triangular, with a relaxed internal sphincter (see the image below).
 A characteristic bladder in prune belly syndrome with vertical orientation, wide trigone, and a urachal remnant. The urethra shows elongation of the posterior urethra with a triangular deformity of the prostatic urethra related to the absent posterior lobe of the prostate.
A characteristic bladder in prune belly syndrome with vertical orientation, wide trigone, and a urachal remnant. The urethra shows elongation of the posterior urethra with a triangular deformity of the prostatic urethra related to the absent posterior lobe of the prostate.
-
Urethra: A wide, long posterior urethra is seen, along with a utricular remnant. The posterior urethra may be triangular in appearance as a result of the absence of the posterior lobe of the prostate. Corporal absence may result in megalourethra of the anterior urethra, giving it a fusiform appearance (see the image below).
-
Cryptorchidism: The testes are in the abdomen or inguinal canals. Often, the testes appear hypoplastic, although they may be of normal size.




For those who have access to nuclear radiology, a scan using a cortical agent such as 99mTc DMSA is useful in assessing renal function. Radiopharmaceuticals that are excreted by tubular secretion such as 99mTc mercaptoacetyltriglycerine (MAG-3) or glomerular filtration such as diethylenetriamine pentaacetic acid (DTPA) may be helpful in visualizing the kidneys and collecting systems.
Computed Tomography
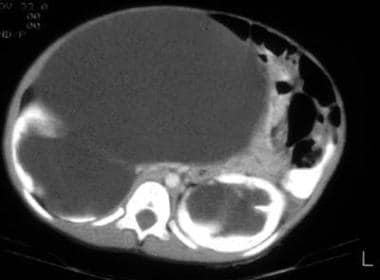
Findings of prune belly syndrome on CT include a broad flabby-appearing abdomen, absence of the musculature of the abdomen, hydronephrosis, and tortuous dilated ureters and bladder. [17]
(See the image below.)
On CT, the ureter in this patient with prune belly syndrome fills the entire abdomen.
Ultrasonography
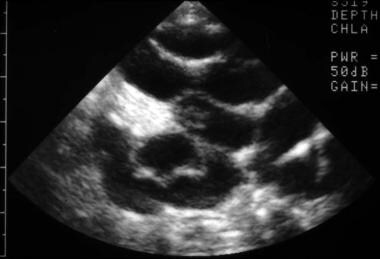
Ultrasonography of the kidneys shows diffusely hyperechoic parenchyma, small parenchymal cysts, clubbed dysplastic calyces, and markedly tortuous ureters; these findings are sufficient to make the diagnosis of prune belly syndrome. The increased echogenicity of the parenchyma is an indicator of underlying dysplasia of the renal tissue during early differentiation and maturation. The bladder is usually large and thick-walled. Angled outlet views may show the dilated prostatic urethra, which is difficult to differentiate from posterior urethral valves by ultrasonography alone. [18, 19, 20, 21, 22]
(See the images below.)
Ultrasound examination of the kidneys shows bilateral hyperechoic kidneys with poor development of the calyces and dilated tortuous ureters.
 High-detail sonogram of an involved kidney shows a hyperechoic cortex, a dysplastic collecting system, and cortical cysts.
High-detail sonogram of an involved kidney shows a hyperechoic cortex, a dysplastic collecting system, and cortical cysts.
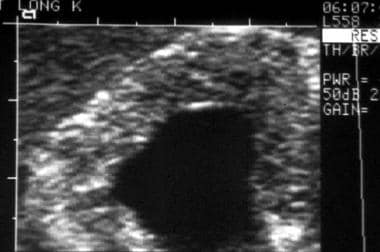
 In prune belly syndrome, an abdominal sonogram usually shows dilated ureters filling the entire abdomen.
In prune belly syndrome, an abdominal sonogram usually shows dilated ureters filling the entire abdomen.
 Note the dilated and hypotonic ureters filling the abdomen in an infant with prune belly syndrome.
Note the dilated and hypotonic ureters filling the abdomen in an infant with prune belly syndrome.
Degree of confidence
On ultrasonography, prune belly syndrome has a characteristic appearance. Although a firm diagnosis may usually be made on the basis of the combination of the clinical examination and US findings, in cases in which abdominal thinning is mild, the diagnosis may be less certain. In such cases, a voiding cystourethrogram may reveal the characteristic urethral appearance.
The diagnosis of prune belly syndrome is made in utero using ultrasonography. In the neonate, the diagnosis is made on the basis of characteristic clinical findings. The diagnosis should be suspected in the fetus when US imaging reveals a characteristic enlarged bladder, dilated ureters, and an abnormal abdominal wall. However, the same constellation of US findings can signal posterior urethral valves with severe hydroureteronephrosis; thus, as a cautionary measure, the diagnosis should not be declared with certainty for either condition.
Megacystis-microcolon syndrome may have an appearance that is almost identical to that of prune belly syndrome; however, in megacystis-microcolon syndrome, the bladder is smoother and larger than in prune belly syndrome. Megacystis-microcolon syndrome has a marked female preponderance.
-
The abdomen of an infant with prune belly syndrome shows marked distention of the abdomen and bulging flanks secondary to a large urinary system and the absence of abdominal wall musculature.
-
Note the small lung volumes and constriction of the upper thorax. Flaring of the lower ribs secondary to distention of the abdomen is seen. Infants with prune belly syndrome may develop severe respiratory distress secondary to the thoracic limitation.
-
Ultrasound examination of the kidneys shows bilateral hyperechoic kidneys with poor development of the calyces and dilated tortuous ureters.
-
High-detail sonogram of an involved kidney shows a hyperechoic cortex, a dysplastic collecting system, and cortical cysts.
-
In prune belly syndrome, an abdominal sonogram usually shows dilated ureters filling the entire abdomen.
-
On CT, the ureter in this patient with prune belly syndrome fills the entire abdomen.
-
Infants with prune belly syndrome show early and marked bilateral vesicoureteral reflux. Significantly more dilatation of the lower ureters exists.
-
A characteristic bladder in prune belly syndrome with vertical orientation, wide trigone, and a urachal remnant. The urethra shows elongation of the posterior urethra with a triangular deformity of the prostatic urethra related to the absent posterior lobe of the prostate.
-
Typical urethra of prune belly syndrome
-
Note the dilated and hypotonic ureters filling the abdomen in an infant with prune belly syndrome.
-
Both prebirth and postnatally, the motion of the diaphragm is restricted by the large size of the abdomen. Because of this effect, most infants with prune belly syndrome have hypoplastic lungs.



