Practice Essentials
The neurofibromatoses are a group of 3 heterogeneous disorders: neurofibromatosis type 1 (NF1), NF2, and schwannomatosis, with NF1 being the most common of the 3, as well as one of the most frequent disorders for cancer predisposition of the nervous system. NF is an autosomal dominant disorder, probably of neural crest origin, that affects all 3 germinal layers; therefore, it can involve any organ system. [1] NF can be discrete cutaneous, subcutaneous discrete, nodular plexiform, or diffuse plexiform. [2]
Patients with NF1 are at increased risk for several malignancies, including gastrointestinal stromal tumors and malignant peripheral nerve sheath tumors (PNSTs). [3] Malignant transformation of PNSTs is the leading cause of mortality in patients with NF1. PNSTs transform into malignant tumors in 8-13% of NF1 patients and contribute to increased mortality. [4]
NF is not a single entity but a group of heterogeneous multisystemic neurocutaneous disorders involving both neuroectodermal and mesenchymal derivatives (see the images below). The National Institutes of Health (NIH) Consensus Development Conference has defined 2 distinct types: neurofibromatosis type 1 (NF1; previously known as von Recklinghausen disease or generalized neurofibromatosis), which affects 85% of patients, and neurofibromatosis type 2 (NF2; previously known as central or bilateral acoustic neuromas/vestibular schwannomas), which affects 10% of patients. [5, 6, 7]
 Frontal skull radiograph in a patient with NF1 shows asymmetry of the orbits but a normal sphenoid ridge.
Frontal skull radiograph in a patient with NF1 shows asymmetry of the orbits but a normal sphenoid ridge.
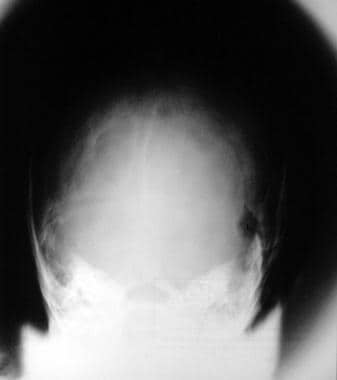 Plain radiograph in a patient with NF1 shows a left lambdoid defect (same patient as in the previous image).
Plain radiograph in a patient with NF1 shows a left lambdoid defect (same patient as in the previous image).
Neurofibromas may affect any organ in the body. Discrete cutaneous and subcutaneous neurofibromas may develop at any time in life, but they occur infrequently before puberty. The total number of neurofibromas seen in adults with NF1 varies from a few to hundreds or even thousands. Additional cutaneous and subcutaneous neurofibromas continue to develop throughout life, although the rate of appearance may vary greatly from year to year.
Clinical manifestations
Many women experience a rapid increase in the number and size of neurofibromas during pregnancy. Although the course of the pregnancy is normal in most women with NF1, serious complications can occur. Hypertension may first become symptomatic or, if preexisting, may become greatly exacerbated during pregnancy. Large pelvic or genital neurofibromas can complicate delivery, and cesarean delivery appears to be necessary more often in women with NF1 than in other women. [8]
Hypertension is frequent in patients with NF1 and may develop at any age. In most patients, the hypertension is essential, but vascular dysplasia can occur in association with NF1 and may produce renal artery stenosis, coarctation of the aorta, or other vascular lesions associated with severe hypertension in adult patients with NF1. [9, 10, 11] Pheochromocytoma can cause severe hypertension in patients with NF1. Malignant neoplasms can occur in patients with NF1 at any age.
Intracranial manifestations of NF1 include development of optic pathway gliomas, [12] cerebral gliomas, hydrocephalus, schwannomas of the cranial nerves, vascular dysplasias, hamartomas, craniofacial plexiform neurofibromas, and spongiotic myelinopathy. NF1 can involve the spine, musculoskeletal system, and the gastrointestinal tract, [13, 14, 15] and NF1 is associated with neural crest tumors. [16]
Multisystemic involvement is common, and a variety of problems may present in childhood, [17] including seizures and intellectual compromise, optic and acoustic involvement, intracranial and spinal tumors, and an increased incidence of malignancies, osseous defects and congenital dislocations, oral pathology, endocrine disorders, autonomic involvement, GI tract involvement, hypertension, and vascular anomalies.
Imaging modalities
The preferred examination depends on the clinical problem to be investigated and the organ involved. Although plain radiographs may be sufficient for evaluating skeletal lesions, sonography and MRI may be the investigation of choice for peripheral nerve tumors and tumors of solid intra-abdominal organs or for associated renal artery stenosis. CT and MRI are preferred with spinal or intracranial lesions. Radionuclide scans are useful when functional imaging is needed in associated tumors such as a pheochromocytoma. [18, 19, 20, 21, 22, 23, 24]
Whole-body MRI is the reference standard to identify nerve sheath tumors in NF1, because it provides a comprehensive characterization of the growth pattern, growth dynamics, and extent of nerve sheath tumors. For detection of malignant transformation of nerve sheath tumors, fluorodeoxyglucose (FDG) PET/CT has a sensitivity of up to 100% and a specificity of 77-95%. [22, 25]
Plain radiographs are excellent at showing skeletal abnormalities of both the axial and appendicular skeleton. Similarly, chest radiography remains a useful technique for demonstrating thoracic cage abnormalities and pulmonary fibrosis. For intracranial, intrathoracic, or intra-abdominal pathology, cross-sectional imaging is more appropriate, and the modality chosen is tailored to the problem.
Radiographic findings of NF1 are nonspecific, but a fairly confident diagnosis can be made in the appropriate clinical setting when the index of clinical suspicion is high. Many neurofibromas may not be depicted on plain radiographs. NF shares many skeletal abnormalities with other syndromes; therefore, the differential diagnosis is extensive.
Angiography remains the criterion standard for providing both anatomic and functional information on vascular aneurysms, occlusions, and arteriovenous shunts. Aneurysms and stenoses are depicted well on angiographic images. Although angiography is highly sensitive in the diagnosis of aneurysms and stenoses, findings only occasionally help in specifying the cause.
NIH criteria
The NIH has developed criteria for the diagnosis of NF1 and NF2. [26] The criteria for the diagnosis of NF1 are met in an individual if 2 or more of the following signs are found:
-
Six or more café au lait macules larger than 5 mm in the greatest diameter in prepubertal children and larger than 1.5 cm in postpubertal individuals
-
Two or more neurofibromas of any type or 1 plexiform neurofibroma
-
Multiple freckles (Crowe sign) in the axillary or inguinal region
-
A distinctive osseous lesion, such as sphenoid dysplasia or thinning of long bone cortex, with or without pseudoarthrosis
-
Optic glioma
-
Two or more iris hamartomas (Lisch nodules) seen on slitlamp or biomicroscopy examination
-
A first-degree relative (parent, sibling, offspring) with NF1, as diagnosed by using the above criteria.
However, the NIH criteria are often insufficient for diagnosis of NF1 in young children who have multiple café au lait spots, no other NF1 features, and no family history of NF1. The overwhelming majority of these children are later diagnosed with NF1 because many of the features are rare in infancy but increase in frequency with age.
Radiography
Skull
Many skull abnormalities are well demonstrated on plain radiographs (see the images below). These include macrocephaly, absence of the greater and lesser wings of the sphenoid, absence of the orbital floor, hypoplasia of the lesser wings of the sphenoid, enlarged orbits, enlargement of cranial foramina, enlargement of orbital margins, sclerosis in the vicinity of the optic foramen (optic nerve sheath meningioma), facial asymmetry, hypoplasia of the paranasal sinuses, mandibular abnormalities, mandibular hypoplasia with flattening of the external contour, thinning of the ramus, coronoid hyperplasia, widening of the lateral and medial coronoid spaces, and calvarial defects adjacent to the lambdoid suture.
Frontal skull radiograph in a patient with NF1 shows asymmetry of the orbits but a normal sphenoid ridge.
Plain radiograph in a patient with NF1 shows a left lambdoid defect (same patient as in the previous image).
Multiple frontobasal osseomeningeal defects causing cerebrospinal fluid (CSF) rhinorrhea and meningoencephalocele can occur, and the osseous defects may be depicted on plain radiographs.
Chest
Plain radiographic findings include inferior rib notching, twisted and ribbonlike ribs in the upper thoracic cage, posterior mediastinal masses secondary to intrathoracic meningoceles, mediastinal and lung masses secondary to neurofibromas, and dumbbell neurofibromas (see the image below).
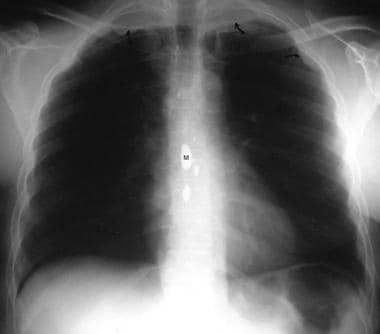 Chest radiograph in a 56-year-old man with NF1 shows apical neurofibromas and ribbon or notched ribs. Note the myodil within the spinal canal from a previous myelography performed because of previous spinal root problems. Myodil or Pantopaque (iophendylate) is an oily contrast medium that was used for myelography in the 1960s and 1970s, but its use was abandoned because of the risk of arachnoiditis.
Chest radiograph in a 56-year-old man with NF1 shows apical neurofibromas and ribbon or notched ribs. Note the myodil within the spinal canal from a previous myelography performed because of previous spinal root problems. Myodil or Pantopaque (iophendylate) is an oily contrast medium that was used for myelography in the 1960s and 1970s, but its use was abandoned because of the risk of arachnoiditis.
Reported changes of lung parenchyma include progressive pulmonary interstitial fibrosis leading to formation of bullae and honeycomb lung (see the image below).
 Chest radiograph in a 62-year-old patient with NF1 shows interstitial fibrosis in the middle and lower zones. Note the multiple surface neurofibromas.
Chest radiograph in a 62-year-old patient with NF1 shows interstitial fibrosis in the middle and lower zones. Note the multiple surface neurofibromas.
The incidence of spontaneous pneumothorax and hemothorax is increased. Changes of interstitial lung disease and pulmonary hypertension may be seen, such as dilatation/enlargement of the central pulmonary arteries and peripheral pruning of vessels.
Spine
A sharply angled kyphoscoliosis centered at the thoracolumbar junction is seen in 50% of patients. The kyphosis is more pronounced than the scoliosis, and the incidence increases with advancing age. Enlargement of the intervertebral foramina, scalloping of the vertebral bodies (anterior, posterior, lateral), hypoplasia of the vertebral pedicles, wedged-shaped vertebrae, spondylolisthesis, spinal clefts, osteolysis, and spindling of the transverse processes may be depicted. Spinal fusion may be complicated by pseudoarthrosis and curve progression. Spinal segments may be unstable, leading to subluxation or dislocation. [27]
Appendicular skeleton
Bowing or an S-shaped deformity of long bones, hyperplasia or hypoplasia of long and short bones, pseudoarthrosis, erosions, periosteal dysplasia, intramedullary longitudinal osteosclerotic streaks, single or multiple cystic bone lesions, and focal gigantism may be depicted. (See the images below.)
 (Left) Plain radiograph of the left forearm in a 15-year-old boy shows hypoplasia and deformity of the radius and ulna. Note the intramedullary sclerotic streaks within the radius and periosteal dysplasia. (Right) Compare these findings with the normal right forearm, and note the unrelated exostosis of the distal radius.
(Left) Plain radiograph of the left forearm in a 15-year-old boy shows hypoplasia and deformity of the radius and ulna. Note the intramedullary sclerotic streaks within the radius and periosteal dysplasia. (Right) Compare these findings with the normal right forearm, and note the unrelated exostosis of the distal radius.
 Plain radiograph of the pelvis in a 28-year-old woman shows gross deformity of the left hemipelvis and the left upper femur.
Plain radiograph of the pelvis in a 28-year-old woman shows gross deformity of the left hemipelvis and the left upper femur.
Joint abnormalities reported include protrusio acetabuli, dislocation of the hip, dislocation of the radius and ulna, absence of a patella, and neuropathic arthropathy of the knee.
GI tract
Abdominal involvement in NF1 has been described, including neurofibromas within the stomach, small and large bowels, and rectum. Barium series may show intraluminal mass lesions due to a neurofibroma indistinguishable from other polypoid lesions.
Intussusception of the bowel may be present with intestinal obstruction. Rarely, bowel obstruction simulating Hirschsprung disease may occur, secondary to plexiform neurofibroma of the colon.
Plexiform neurofibromas may cause a mass effect on adjacent barium-filled bowel loops. Small-bowel leiomyoma, small-bowel adenocarcinoma with neuroendocrine function, stromal tumors, and carcinoid tumors are other reported associations. Pseudo-obstruction has been reported.
A barium small-bowel series (see the images below) may show features consistent with malabsorption resulting from protein-losing enteropathy.
 Upper GI barium series in a 56-year-old woman with NF1 shows multiple filling defects along the greater curve of the stomach due to neurofibromas. Note the multiple subcutaneous neurofibromas in the right upper quadrant.
Upper GI barium series in a 56-year-old woman with NF1 shows multiple filling defects along the greater curve of the stomach due to neurofibromas. Note the multiple subcutaneous neurofibromas in the right upper quadrant.
 Upper GI barium series in a 56-year-old woman shows multiple polypoid filling defects throughout the small bowl due to neurofibromas (same patient as in the previous image). Note the subcutaneous neurofibromas projected over the right hypochondrium.
Upper GI barium series in a 56-year-old woman shows multiple polypoid filling defects throughout the small bowl due to neurofibromas (same patient as in the previous image). Note the subcutaneous neurofibromas projected over the right hypochondrium.
Biliary strictures and bile duct intraluminal neurofibromas are rarely associated and may be revealed on percutaneous cholangiography or endoscopic retrograde cholangiopancreatography (ERCP). [28]
Urinary tract
The renal collecting system and bladder may be intrinsically involved by neurofibromas or extrinsically compressed or displaced by neurofibromas.
Plain radiography has little to contribute besides showing a soft-tissue mass, but intravenous urography may provide useful information regarding the nature and site of obstruction and function.
Computed Tomography
Peripheral soft-tissue NF
CT scans demonstrate solid fusiform masses in the distribution of nerves, with central areas of low attenuation and calcification. These masses may present in the paravertebral, laryngeal, mediastinal, abdominal, and pelvic/ischiorectal fossae. The masses usually are well defined, with attenuation values of approximately 30-40 Hounsfield units (HU). CT has a role in the investigation of thoracic, abdominal, and pelvic complications of NF1.
Plexiform neurofibromas are depicted as widespread sheets of nodular tissue, with attenuation values identical to the fusiform form (30-40 HU).
Paraspinal neurofibromas may be seen at every level, may vary in size, may be dumbbell shaped, or may comprise fusiform/spherical soft-tissue masses with attenuation values of approximately 20-30 HU. Dumbbell-shaped neurofibromas may enlarge the exiting foramina.
A characteristic appearance may be seen of mesenteric plexiform neurofibromas trapping mesenteric fat within an entangled network, with attenuation values of approximately 15-30 HU. Nonneoplastic cerebral and cerebellar calcification and choroid plexus calcification are depicted well on cranial CT scans.
Hydrocephalus in NF1 may be due to benign aqueduct stenosis or a glioma of the tectum/tegmentum of the mesencephalon (see the image below).

Intracranial nerve sheath tumors are not depicted as well on CT scans as they are on MRI, but associated bone erosions are seen well on CT. Meningiomas with associated changes in the calvarium/skull are depicted well.
Dural calcifications may be seen, especially at vertex. Macrocephaly due to hydrocephalus or increased white matter volume may be seen.
Extrinsic bladder involvement, intrinsic infiltrative processes, or extrinsic compression of the renal collecting system by a neurofibroma may be revealed on CT scans as masses of low attenuation.
CT scans and MRIs are excellent at depicting most primary lesions and associated tumors and complications of NF1. Some pathology is better imaged by using MRI, such as optic nerve glioma and intraspinal abnormalities. However, even with optic nerve gliomas, osseous erosions may be depicted better on CT scans. [29, 30, 19] Neurofibromas can occur as an isolated anomaly and in association with NF2. Certain congenital bone lesions may mimic bone involvement associated with NF1, such as fibrous dysplasia. A number of syndromes can mimic NF1.
Magnetic Resonance Imaging
Brain anomalies
Approximately 15% of patients with NF1 display a brain anomaly on MRI. The lesions are often multiple in characteristic locations, such as the pons, cerebellar white matter, midbrain, splenium of the corpus callosum, and internal capsule. [31] Cerebral volumetric abnormalities are some of the most often observed CNS abnormalities in NF1. In a study of 15 NF1 patients (mean age, 12.9 yr) and 18 healthy controls (mean age, 13.8 yr) who underwent 3T MRI scanning, larger volumes of all subcortical regions were found in NF1 patients as compared to controls. In addition, patients showed decreased gray matter density in midline regions of the frontal and parietal lobes and larger total white matter volume. Also, larger left putamen volume and larger total white matter volume were associated with more social problems and poorer executive functioning; larger right amygdala volume was associated with poorer executive functioning and autistic mannerisms; and smaller precentral gyrus gray matter density was associated with more social problems. [23]
MRI is the modality of choice for imaging neural sheath tumors, which can be demonstrated by following the course of the nerve from which the tumor arises. Intracranial neural sheath tumors are isointense to brain tissue on T1-weighted images and hyperintense to brain tissue on T2-weighted images. Tumors enhance intensely following contrast administration. Nerve sheath tumors are the most common intradural neoplasms. Schwannomas usually arise from the dorsal sensory root. They are almost always solitary and sporadic in NF1, but multiple schwannomas occur in NF2. Intradural neurofibromas are almost always multiple in NF1.
In a study by Well et al of 26 patients with NF1 and suspicion of malignant transformation of peripheral nerve sheath tumors (PNSTs), diffusion-weighted MRI showed better diagnostic performance than morphologic features and allowed accurate differentiation between benign and malignant peripheral nerve sheath tumors. Malignant PNSTs demonstrated significantly lower diffusivity than benign PNSTs. [4]
Tumors tend to be smoothly marginated. Larger tumors are heterogeneous. Tumors occasionally present at the base of the brain and may spread through the basal foramina.
Intraparenchymal brain abnormalities include isointense or hyperintense foci on T2-weighted images in the cerebellar white matter, dentate nucleus, basal ganglia, periventricular white matter, optic nerve, and optic pathways. These lesions are isointense on T1-weighted images and usually have no mass effect. (The lesions are classed as hamartomas but are probably demyelinating lesions because they may resolve.) They become visible between ages 2 and 10 years, then regress by the second decade. If the T2 lesions show enhancement, glioma development should be suspected.
Rarely, hyperintensities and mild mass effect have been reported in the globus pallidus on T1-weighted images.
Optic gliomas, which are the most common intracranial lesion in NF1, and gliomas of other parts of the brain may be demonstrated (see the images below). [21, 22, 23, 24]
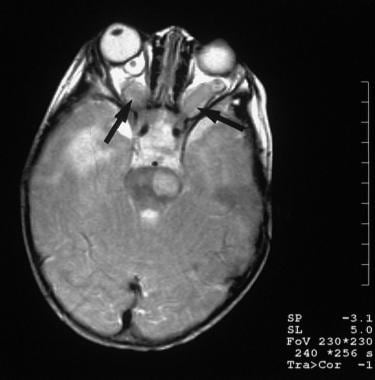 A 7-year-old girl with a family history of NF1 had been blind for 18 months. T2-weighted transaxial MRI shows bilateral optic nerve gliomas (arrows), as well as a right temporal lobe and left brainstem lesions, which may represent additional gliomas or spongiform white matter changes of NF1.
A 7-year-old girl with a family history of NF1 had been blind for 18 months. T2-weighted transaxial MRI shows bilateral optic nerve gliomas (arrows), as well as a right temporal lobe and left brainstem lesions, which may represent additional gliomas or spongiform white matter changes of NF1.
 T1-weighted MRI in a 7-year-old girl with a family history of NF1 who had been blind for 18 months shows bilateral optic nerve gliomas (arrows) (same patient as in the previous image).
T1-weighted MRI in a 7-year-old girl with a family history of NF1 who had been blind for 18 months shows bilateral optic nerve gliomas (arrows) (same patient as in the previous image).
A retrospective analysis of 826 individuals with NF1 (402 females, 424 males) aged 1-9 years who were screened for optic pathway gliomas with brain/orbital MRI confirmed that chiasmatic and postchiasmatic optic pathway gliomas in children with NF1 have the highest risk for progression and vision loss. Children with negative brain and orbital MRI screening at age 15 months or later did not develop symptomatic optic pathway gliomas. [24]
Gliomatosis cerebri may be seen, which is an unusual confluence of astrocytomas. Dural calcifications may be seen, especially at vertex. Hydrocephalus in NF1 may be due to benign aqueduct stenosis or a glioma of tectum/tegmentum of the mesencephalon. Macrocephaly due to hydrocephalus or increased white matter volume may be seen.
Schwannomas and neurofibromas
Although schwannomas and neurofibromas are histologically different, they exhibit similar MRI appearances. Both schwannomas and neurofibromas are hypointense or mildly hypointense compared to the spinal cord on T1-weighted images and are heterogeneously hyperintense on T2-weighted images. The tumors may extend into the neural foramina. Within schwannomas, areas of hypointensity due to collagen deposition, hemorrhage, and densely packed Schwann cells are frequently seen. After the administration of contrast material, peripheral enhancement of schwannomas predominates.
Neurofibromas enhance more homogeneously. Enhancement patterns and T2-weighted images can help differentiate schwannomas from meningiomas, but the same confidence cannot be transferred to differentiating schwannomas from neurofibromas.
MRI allows noninvasive identification of intradural neurofibromas and helps determine their relationship to the neural foramina, canal, and thecal sac spinal cord. The target sign (bright on T2, with dark collagen centrally) is highly suggestive of a peripheral neurofibroma on MRI. It may be seen with plexiform neurofibromas as well. Paraspinal neurofibromas may be dumbbell shaped, fusiform, or spherical (see the images below). They are slightly hyperintense relative to muscle on T1-weighted images, with a hyperintense periphery and a hypointense core on T2-weighted images.
 Sagittal T1-weighted unenhanced MRI scan in a 28-year-old woman shows dural ectasia and a large lobulated anterior sacral meningocele (M).
Sagittal T1-weighted unenhanced MRI scan in a 28-year-old woman shows dural ectasia and a large lobulated anterior sacral meningocele (M).
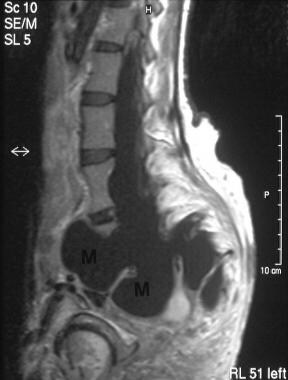 Sagittal T2-weighted MRI in a 28-year-old woman shows dural ectasia and a large lobulated anterior meningocele (same patient as in the previous image).
Sagittal T2-weighted MRI in a 28-year-old woman shows dural ectasia and a large lobulated anterior meningocele (same patient as in the previous image).
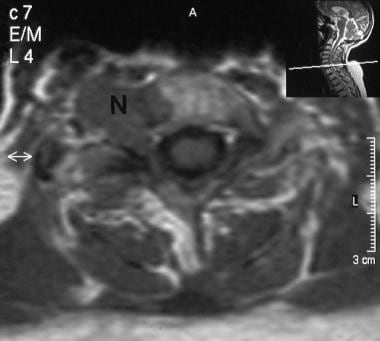 A 66-year-old woman with NF1 presented with paresthesia down the right arm. T1-weighted transaxial MRI through the cervical spine shows a low-signal-intensity mass extruding through the right foraminal canal at the C5-6 vertebral level; the mass appears to be eroding the vertebral body. The final diagnosis was a neurofibroma.
A 66-year-old woman with NF1 presented with paresthesia down the right arm. T1-weighted transaxial MRI through the cervical spine shows a low-signal-intensity mass extruding through the right foraminal canal at the C5-6 vertebral level; the mass appears to be eroding the vertebral body. The final diagnosis was a neurofibroma.
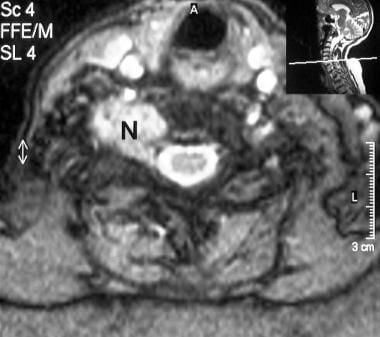 T2-weighted transaxial MRI in a 66-year-old woman shows a moderately hyperintense neurofibroma (N) (same patient as in the previous image).
T2-weighted transaxial MRI in a 66-year-old woman shows a moderately hyperintense neurofibroma (N) (same patient as in the previous image).
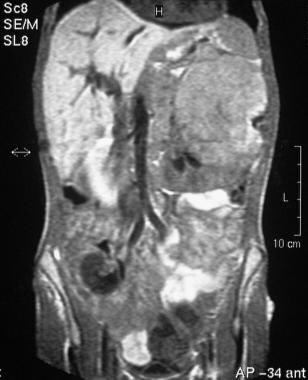 T1-weighted coronal MRI of the abdomen in a 28-year-old man shows a low-signal dumbbell-shaped right iliac fossa tumor, confirmed to be a neurofibroma at laparotomy. The patient also had sickle cell trait and presented with hematuria from a left-sided medullary cell renal carcinoma.
T1-weighted coronal MRI of the abdomen in a 28-year-old man shows a low-signal dumbbell-shaped right iliac fossa tumor, confirmed to be a neurofibroma at laparotomy. The patient also had sickle cell trait and presented with hematuria from a left-sided medullary cell renal carcinoma.
Other manifestations
A lateral thoracic meningocele, which is known to be associated with NF1, is depicted well on MRIs and is seen as a CSF-filled sac extending through a widened neural foramina.
Other CNS abnormalities associated with NF1 are depicted well on MRIs and include prominent CSF spaces, arachnoid cysts, arachnoid pouches, frontobasal meningocele, craniofacial plexiform neurofibromas, and intracranial lipoma.
Extrinsic bladder involvement, an intrinsic infiltrative process, and extrinsic compression of the renal collecting system by a neurofibroma are depicted well, with a markedly increased signal within the compressing mass on T2-weighted images and a slightly increased signal intensity on T1-weighted images relative to muscle.
Cardiovascular abnormalities, such as a superior vena cava aneurysm, obstruction, lymphatic obstruction, left atrial wall aneurysm, aneurysm of the coronary arteries, aneurysm of other major or minor vessels, and stenoses of cranial, renal, celiac axis, and superior mesenteric arteries, are depicted well with magnetic resonance angiography (MRA) or contrast-enhanced dynamic MRA.
Degree of confidence
MRI is the modality of choice because the course of the nerve from which the tumor arises can be detected, and MRI can depict neural sheath tumors. MRI also depicts optic nerve gliomas better than CT. [29, 30, 19]
Unidentified bright objects typically disappear with age, in the setting of children with NF1. However, it is often difficult to distinguish unidentified bright objects from low-grade glioma without tissue diagnosis. Ostendorf and associates have described a 4-year-old boy with NF1 who had an asymptomatic optic glioma and right basal ganglia unidentified bright object. The child developed a left hemiparesis with hyperreflexia over the course of a year. MRI revealed a cystlike mass in the region of his previously identified T2 hyperintensity. Unidentified bright objects often do not become cystic with associated mass effect. Coupled with the development of new neurologic signs, these MRI features are worrisome for neoplasm in a patient with NF1. [6]
T2-weighted high-signal intensities within the brain recognized as unidentified bright objects on MRI are a common finding in children with NF1. Unidentified bright objects are most prevalent between ages 4 and 12 years. Unidentified bright objects are particularly common in the globus pallidus and the cerebellum. In this subset of patients, unidentified bright objects do not show any significant change despite a worsening in clinical symptoms. [32]
Schwannomas and neurofibromas cannot always be differentiated. When solitary, the tumor usually is regarded as a schwannoma; when multiple, tumors usually are diagnosed as neurofibromas.
Ultrasonography
Solitary neurofibromas are mostly hyperechoic with coarse internal echoes and lobulated margins. Nonplexiform neurofibromas in NF1 appear as hypoechoic fusiform masses, and although they do not have a histologic capsule, they present with relatively regular and well-defined margins. [33] (See the image below.)
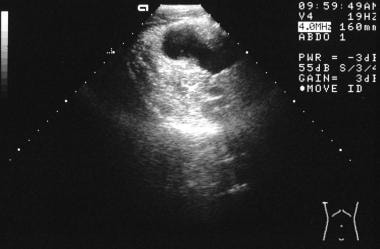 Axial sonogram through the right iliac fossa in a 28-year-old man with NF1 shows a hypoechoic dumbbell-shaped neurofibroma.
Axial sonogram through the right iliac fossa in a 28-year-old man with NF1 shows a hypoechoic dumbbell-shaped neurofibroma.
Small intratumoral cystic areas due to myxoid degeneration may be present in schwannomas. When a sudden increase in tumor size is detected, malignant transformation should be considered.
Paraspinal neurofibromas may appear as well-circumscribed cylindrical lesions. Abdominal involvement that may be depicted on sonography includes NF and tumor growth in the liver, mesentery, and the retroperitoneum, in addition to mesenteric leiomyomatosis and gastric and bowel tumors.
Biliary obstruction may be demonstrated on ultrasound images, and tumor spread into the liver along the portal vein has been shown as infiltrative hypoechoic masses around the porta hepatis and intrahepatic portal branches. Similarly, obstructive uropathy caused by neurofibroma may be depicted on ultrasound images.
Duplex color and spectral Doppler ultrasonography are useful diagnostic modalities for revealing the vascular complications of NF1, such as aneurysms and stenoses.
Degree of confidence
The diagnosis of nerve sheath tumors with sonography depends on depiction of a mass along the presumed course of a nerve in association with neurologic signs. Thus, sonography is reliable only when a definite relationship can be demonstrated between a mass and a nerve origin. [19]
Peripheral lymphadenopathy may superficially resemble neurofibromas. Lesions within other solid or cystic intra-abdominal organs need to be differentiated from other masses.
Nuclear Imaging
Radionuclide isotope bone scans can be useful in the investigation of intraosseous lesions and pseudofractures because differentiation from metastases may be possible. Technetium-99m diethylenetriamine pentaacetic acid (DTPA) has been shown to accumulate in benign soft-tissue tumors of NF. Positron emission tomography has been used to image the uptake of fluorodeoxyglucose (FDG) in the malignant transformation of a neurofibroma. [34, 35, 36, 37, 21, 22]
The role of nuclear medicine is complementary, and the findings are seldom diagnostic.
Although radionuclide scans are sensitive in detecting bone pathology, the appearances are nonspecific, and positive findings may occur in a variety of bone pathologies.
NF1 is associated with peripheral nerve sheath tumors, the majority being benign neurofibromas. However, malignant peripheral nerve sheath tumors occur with a 10% lifetime risk in patients, in the setting of NF1, often developing within a neurofibroma. With a clinical suspicion of a malignant peripheral nerve sheath, imaging with MRI and FDG positron emission tomography (PET) is performed for potential malignancy. [21]
In a study of F-18-FDG PET/CT used in individuals with NF1, malignant peripheral nerve sheath tumors demonstrated a significantly higher whole-body malignant tumor volume and whole-body total lesion glycolysis than benign peripheral nerve sheath tumors. [21]
Ahlawat et al have reported a pitfall in the use of metabolic imaging, which has the potential for false-positive findings. The authors describe a patient with NF1 who had a malignant nerve sheath tumor and a second schwannoma, both of which showed FDG uptake. [38]
-
Frontal skull radiograph in a patient with NF1 shows asymmetry of the orbits but a normal sphenoid ridge.
-
Plain radiograph in a patient with NF1 shows a left lambdoid defect (same patient as in the previous image).
-
(Left) Plain radiograph of the left forearm in a 15-year-old boy shows hypoplasia and deformity of the radius and ulna. Note the intramedullary sclerotic streaks within the radius and periosteal dysplasia. (Right) Compare these findings with the normal right forearm, and note the unrelated exostosis of the distal radius.
-
Chest radiograph in a 56-year-old man with NF1 shows apical neurofibromas and ribbon or notched ribs. Note the myodil within the spinal canal from a previous myelography performed because of previous spinal root problems. Myodil or Pantopaque (iophendylate) is an oily contrast medium that was used for myelography in the 1960s and 1970s, but its use was abandoned because of the risk of arachnoiditis.
-
Chest radiograph in a 62-year-old patient with NF1 shows interstitial fibrosis in the middle and lower zones. Note the multiple surface neurofibromas.
-
Plain radiograph of the pelvis in a 28-year-old woman shows gross deformity of the left hemipelvis and the left upper femur.
-
Sagittal T1-weighted unenhanced MRI scan in a 28-year-old woman shows dural ectasia and a large lobulated anterior sacral meningocele (M).
-
Sagittal T2-weighted MRI in a 28-year-old woman shows dural ectasia and a large lobulated anterior meningocele (same patient as in the previous image).
-
A 66-year-old woman with NF1 presented with paresthesia down the right arm. T1-weighted transaxial MRI through the cervical spine shows a low-signal-intensity mass extruding through the right foraminal canal at the C5-6 vertebral level; the mass appears to be eroding the vertebral body. The final diagnosis was a neurofibroma.
-
T2-weighted transaxial MRI in a 66-year-old woman shows a moderately hyperintense neurofibroma (N) (same patient as in the previous image).
-
CT scan through the orbits in a patient with NF1 shows a right optic glioma.
-
A 7-year-old girl with a family history of NF1 had been blind for 18 months. T2-weighted transaxial MRI shows bilateral optic nerve gliomas (arrows), as well as a right temporal lobe and left brainstem lesions, which may represent additional gliomas or spongiform white matter changes of NF1.
-
T1-weighted MRI in a 7-year-old girl with a family history of NF1 who had been blind for 18 months shows bilateral optic nerve gliomas (arrows) (same patient as in the previous image).
-
Axial sonogram through the right iliac fossa in a 28-year-old man with NF1 shows a hypoechoic dumbbell-shaped neurofibroma.
-
T1-weighted coronal MRI of the abdomen in a 28-year-old man shows a low-signal dumbbell-shaped right iliac fossa tumor, confirmed to be a neurofibroma at laparotomy. The patient also had sickle cell trait and presented with hematuria from a left-sided medullary cell renal carcinoma.
-
Upper GI barium series in a 56-year-old woman with NF1 shows multiple filling defects along the greater curve of the stomach due to neurofibromas. Note the multiple subcutaneous neurofibromas in the right upper quadrant.
-
Upper GI barium series in a 56-year-old woman shows multiple polypoid filling defects throughout the small bowl due to neurofibromas (same patient as in the previous image). Note the subcutaneous neurofibromas projected over the right hypochondrium.









