Practice Essentials
An osteoblastoma is an uncommon primary neoplasm of the bone that has clinical and histologic manifestations that are similar to those of an osteoid osteoma; therefore, some experts consider the 2 lesions to be variants of the same disease, with osteoblastoma representing a giant osteoid osteoma. However, an aggressive type of osteoblastoma has been recognized, making the relationship between the lesions less clear. Osteoblastoma accounts for about 1% of all primary bone tumors and 3% of all benign bone tumors. Approximately 30-40% of cases occur in the posterior elements of the spine and the sacrum, with other common locations including the mandible and long tubular bones. Patients with osteoblastoma generally have a good prognosis. [1, 2, 3, 4, 5, 6]
(See the osteoblastoma images below.)
 Lateral radiograph of the cervical spine in a 10-year-old boy. The spinous process of the C3 vertebra is expanded by a mass with ossific matrix.
Lateral radiograph of the cervical spine in a 10-year-old boy. The spinous process of the C3 vertebra is expanded by a mass with ossific matrix.
 T1-weighted gadolinium-enhanced sagittal magnetic resonance image of the spine in a 10-year-old boy. This image reveals contrast enhancement of a mass that is occupying the posterior elements of the C3 vertebra.
T1-weighted gadolinium-enhanced sagittal magnetic resonance image of the spine in a 10-year-old boy. This image reveals contrast enhancement of a mass that is occupying the posterior elements of the C3 vertebra.
 Computed tomography scan of the cervical spine in a 10-year-old boy. This image reveals a lytic lesion that involves the posterior elements of the C3 vertebra. Cortical expansion of the spinous process and an ossified matrix are noted; these findings are typical and classic findings in cases of osteoblastomas.
Computed tomography scan of the cervical spine in a 10-year-old boy. This image reveals a lytic lesion that involves the posterior elements of the C3 vertebra. Cortical expansion of the spinous process and an ossified matrix are noted; these findings are typical and classic findings in cases of osteoblastomas.
Presentation and natural history
Osteoblastoma is typically seen in the second decade of life, with a male predilection. [7] Approximately 40% of all osteoblastomas are located in the spine. [8, 9, 10] The tumors usually involve the posterior elements, and 17% of spinal osteoblastomas are found in the sacrum. The long tubular bones are another common site of involvement, with a preponderance in the lower extremities. Osteoblastoma of the long tubular bones is often diaphyseal, and fewer are located in the metaphysis. Epiphyseal involvement is extremely rare. Other reported sites include the bones of the hands, wrists, feet and ankles [11] ; the skull and facial bones [12, 13, 14, 15, 16, 17] ; the ribs [18, 19] ; and the sternum, clavicles, scapulae, patellae, and pelvis. [20]
Benign osteoblastoma of the cranium affects women slightly more often than men and typically presents in the first 3 decades of life. Cranial osteoblastoma usually presents as a painful, nonmobile, subcutaneous mass or swelling. On CT scan, cranial osteoblastoma generally presents as a well-demarcated, mixed lytic and sclerotic lesion, with enlarged diploe, thinning outer and/or inner tables, and varying degrees of calcification. It is hypointense to isointense on T1-weighted MRI and has variable presentation on T2-weighted MRI. [21]
The etiology of osteoblastoma is unknown. Histologically, osteoblastomas are similar to osteoid osteomas, producing both osteoid and primitive woven bone amidst fibrovascular connective tissue. Although the tumor is usually considered benign, a controversial aggressive variant has been described in the literature, with histologic features similar to those of malignant tumors such as osteosarcomas. [22, 23, 24, 25] FOS expression has been reported in osteoblastomas, which suggests that fluorescence in-situ hybridization (FISH) analysis for FOS rearrangement could be helpful in the diagnosis of cases with worrying histologic features. [26]
Patients with osteoblastomas usually present with pain of several months' duration. In contrast to the pain that is associated with osteoid osteoma, the pain of an osteoblastoma is usually less intense, is usually not worse at night, and is not relieved readily with salicylates. If the lesion is superficial, the patient may have localized swelling and tenderness. Spinal lesions can cause painful scoliosis, although this is less common with osteoblastomas than with osteoid osteomas. In addition, lesions may mechanically interfere with the spinal cord or nerve roots, producing neurologic deficits. [27, 28]
Imaging modalities
The preliminary radiologic workup should consist of radiography at the site of the patient's pain. [29, 30] In most patients, radiographic findings are not diagnostic of osteoblastoma; therefore, further imaging is warranted. Computed tomography (CT) scanning is often necessary to support clinical and conventional radiographic findings that are suggestive of osteoblastoma and to better define the margins of the lesion for potential surgery. [31, 21] CT scans are best used for the further characterization of the lesion with regard to the presence of a nidus and matrix mineralization. [32, 31] A CT scan examination that is performed with the intravenous administration of a contrast agent poses the risk of a patient's allergic reaction to the contrast material.
Magnetic resonance imaging (MRI) aids in the detection of nonspecific reactive marrow and soft-tissue edema. [33, 34] This modality best defines soft-tissue extension, although the finding is not typical of osteoblastoma. The lengthy duration of an MRI examination and a history of claustrophobia in some patients limit the use of MRI. [1, 35]
A single-center retrospective study by Arrigoni et al found MR-guided focused ultrasound (MRgFUS) to be safe and effective for treating intra-articular osteoblastoma with a good acoustic window. [36] MRgFUS has been shown in studies to be able to provide tumor ablation without use of a needle or ionizing radiatio, as well as providing a precise and controlled increase in temperature, delivering small amounts of energy to destroy only the lesion, and avoiding healthy surrounding tissue. [37]
Bone scintigraphy demonstrates abnormal radiotracer accumulation at the affected site, substantiating clinical suspicion, but this finding is not specific for osteoblastoma. [29] In many patients, biopsy is necessary for confirmation of the diagnosis.
Although osteoblastomas demonstrate an increased radiotracer accumulation on bone scans, the tumors' appearance is nonspecific, and it is difficult to differentiate these lesions from those due to other etiologies that involve increased radiotracer accumulation in the bone. Therefore, bone scans are only useful in conjunction with other radiologic studies and are best not used alone.
The major diagnostic problem is in differentiating malignant or aggressive osteoblastoma from osteosarcoma on the basis of the pathologic features because the diagnosis markedly changes treatment in patients.
Most of the medical and/or legal pitfalls that are associated with osteoblastomas result from the often nonspecific radiographic appearance of these tumors. In many patients, analysis of biopsy specimens is necessary for a definitive diagnosis. If a radiologist is asked to perform a biopsy in a suspected osteoblastoma, the orthopedic surgeon should be consulted first.
Radiography
The radiographic appearances of osteoblastomas vary. Occasionally, the osteoblastoma appears as a sclerotic lesion, and in other instances, it appears as a lucent expansile lesion. Findings in as many as 25% of patients may demonstrate features that are suggestive of a malignant process, such as cortical thinning, expansion of the bone, and the presence of a soft-tissue mass. [38]
Radiographic findings are not diagnostic of osteoblastoma in most patients; therefore, further imaging studies are warranted.
Osteoblastomas in the spine usually occur in the posterior elements (see the image below). When a well-defined expansile lesion is identified in this location, a diagnosis of osteoblastoma should always be considered. Approximately 50% of osteoblastomas in the spine contain matrix mineralization.
Lateral radiograph of the cervical spine in a 10-year-old boy. The spinous process of the C3 vertebra is expanded by a mass with ossific matrix.
An osteoblastoma in the skull produces a sharply marginated radiolucent defect that contains central calcification or ossification; this finding is highly suggestive of the diagnosis. Lesions in the mandible are often located near the tooth root.
The varied radiologic appearance of the neoplasm in sites other than the posterior elements of the spine and the skull does not allow a precise diagnosis. The appearance of the lesion may resemble a large osteoid osteoma, with the typical radiographic features of a nidus and a surrounding area of reactive bone. The nidus of an osteoblastoma is larger than that of an osteoid osteoma, with some investigators using 2 cm as a size distinction. If the nidus is eccentrically located in the bone, thick periosteal reaction may be prominent.
(See the images below.)
 Knee radiograph from a 16-year-old boy with lower leg pain. This image reveals a somewhat poorly defined and nonspecific lucent lesion in the proximal tibial metaphysis.
Knee radiograph from a 16-year-old boy with lower leg pain. This image reveals a somewhat poorly defined and nonspecific lucent lesion in the proximal tibial metaphysis.
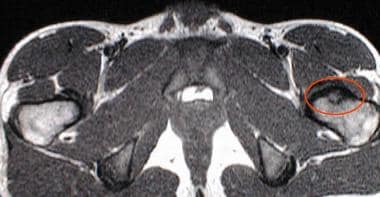
 Radiograph of the left hip in a 14-year-old boy. This image demonstrates a lytic lesion in the intertrochanteric region of the left femur with a faint, diffuse, surrounding sclerosis. The long bones are the second most common location for osteoblastomas.
Radiograph of the left hip in a 14-year-old boy. This image demonstrates a lytic lesion in the intertrochanteric region of the left femur with a faint, diffuse, surrounding sclerosis. The long bones are the second most common location for osteoblastomas.
The lesions may have radiographic features that are similar to those of an aneurysmal bone cyst, eosinophilic granuloma, enchondroma, fibrous dysplasia, chondromyxoid fibroma, or solitary bone cyst. The presence of an osseous matrix within the lesion may suggest an osteoblastoma. In patients in whom osteoblastoma simulates an aggressive tumor, neoplasms such as osteosarcoma and Ewing sarcoma are included in the differential diagnosis.
Osteoblastomas in the long tubular bones may arise from the medullary or cortical bone. These lesions usually appear as geographic lucencies with internal calcification and/or ossification, and they often expand the cortex. The surrounding sclerosis and periostitis, seen in as many as 50% of patients, can simulate an aggressive process and may be misinterpreted as evidence of a malignant neoplasm. Osteoblastomas may be encountered in the small bones of the hands, wrists, feet, and ankles, as well as in the flat bones.
(See the images below.)
 Radiograph of the right shoulder in a 39-year-old woman. This image reveals a large lytic lesion arising in the proximal part of the humerus.
Radiograph of the right shoulder in a 39-year-old woman. This image reveals a large lytic lesion arising in the proximal part of the humerus.
 Oblique view of the ankle. This radiograph reveals a lucent lesion within the talus, an uncommon location for osteoblastomas. Although this appearance is consistent for an osteoblastoma, it is nonspecific.
Oblique view of the ankle. This radiograph reveals a lucent lesion within the talus, an uncommon location for osteoblastomas. Although this appearance is consistent for an osteoblastoma, it is nonspecific.

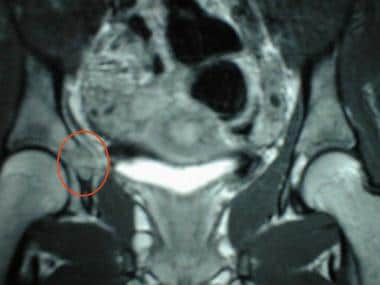
 Anteroposterior radiographic view of the pelvis in a 14-year-old girl who presented with right hip pain. This image reveals a lucent, slightly expansile lesion in the acetabulum.
Anteroposterior radiographic view of the pelvis in a 14-year-old girl who presented with right hip pain. This image reveals a lucent, slightly expansile lesion in the acetabulum.
 Magnified radiographic view of the pelvis in a 14-year-old girl who presented with right hip pain. This image reveals the same lucent, slightly expansile lesion in the acetabulum.
Magnified radiographic view of the pelvis in a 14-year-old girl who presented with right hip pain. This image reveals the same lucent, slightly expansile lesion in the acetabulum.
Computed Tomography
CT scans aid in defining the extent of the osteoblastoma and in detecting the presence of matrix mineralization. CT scan findings may support the diagnosis of osteoblastoma that has been made with the use of plain films, increasing the interpreter's degree of confidence. Some investigators have used CT to guide radiofrequency ablation of osteoblastoma. [39]
(See the images below.)
 The computed tomography scan findings are nonspecific and have a benign appearance in this image.
Computed tomography scan of the cervical spine in a 10-year-old boy. This image reveals a lytic lesion that involves the posterior elements of the C3 vertebra. Cortical expansion of the spinous process and an ossified matrix are noted; these findings are typical and classic findings in cases of osteoblastomas.
The computed tomography scan findings are nonspecific and have a benign appearance in this image.
Computed tomography scan of the cervical spine in a 10-year-old boy. This image reveals a lytic lesion that involves the posterior elements of the C3 vertebra. Cortical expansion of the spinous process and an ossified matrix are noted; these findings are typical and classic findings in cases of osteoblastomas.
CT scans, similar to conventional radiographs, may demonstrate a predominantly osteolytic and expansile lesion, with or without central mineralization. The images may also show a predominantly sclerotic lesion or a mixed lesion.
(See the images below.)
 Computed tomography scan in a 39-year-old woman. This image demonstrates faint matrix mineralization.
Computed tomography scan in a 39-year-old woman. This image demonstrates faint matrix mineralization.
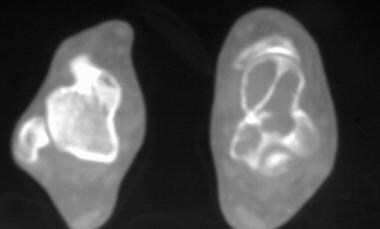
 Axial computed tomography scan of the right hip in a 14-year-old girl. This image reveals small amounts of matrix mineralization and cortical expansion.
Axial computed tomography scan of the right hip in a 14-year-old girl. This image reveals small amounts of matrix mineralization and cortical expansion.
The medullary or cortical location of the tumor can be well defined. Adjacent bony sclerosis, periosteal reaction, or cortical erosion may be demonstrated.
(See the images below.)
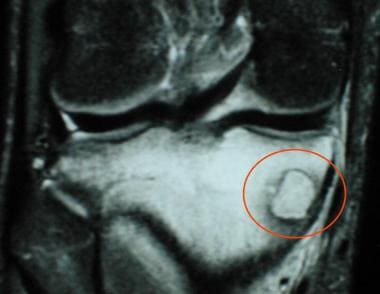
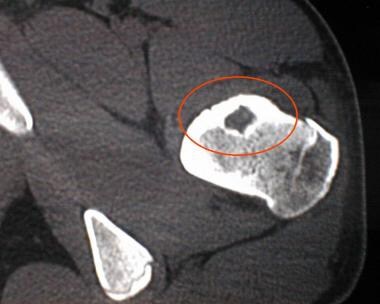 Computed tomography scan of the left proximal femur in a 14-year-old boy. This image reveals a cortically based nidus with surrounding thickened bone.
Computed tomography scan of the left proximal femur in a 14-year-old boy. This image reveals a cortically based nidus with surrounding thickened bone.
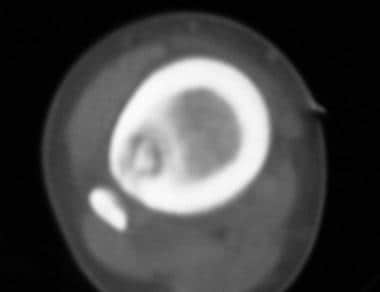 Axial computed tomography scan that was obtained through the tibial diaphysis. This image demonstrates how an osteoblastoma can resemble a large osteoid osteoma, with the typical radiographic features of a central nidus and surrounding reactive bone.
Axial computed tomography scan that was obtained through the tibial diaphysis. This image demonstrates how an osteoblastoma can resemble a large osteoid osteoma, with the typical radiographic features of a central nidus and surrounding reactive bone.
Magnetic Resonance Imaging
Similar to CT scans, MRI examinations can aid in defining the extent of the osteoblastoma, as shown below. Although MRI is useful for delineating the extent of osteoblastomas, the appearance of the tumors is usually nonspecific. MRI findings may lead to an osteoblastoma's appearance mimicking that of a malignancy.
 T1-weighted sagittal magnetic resonance image of the left foot. This image reveals a lesion with low signal intensity in the talus.
T1-weighted sagittal magnetic resonance image of the left foot. This image reveals a lesion with low signal intensity in the talus.
MRI is often superior to CT scanning with regard to the detection of a soft-tissue mass, although this is a relatively uncommon feature of osteoblastomas. A typical osteoblastoma has decreased signal intensity on T1-weighted images. [8]
(See the images below.)
 T1-weighted sagittal magnetic resonance image of the spine in a 10-year-old boy. This image suggests the presence of a mass that involves the posterior elements of the C3 vertebra.
T1-weighted sagittal magnetic resonance image of the spine in a 10-year-old boy. This image suggests the presence of a mass that involves the posterior elements of the C3 vertebra.
 T1-weighted sagittal magnetic resonance image in a 16-year-old boy with lower leg pain. This image demonstrates a focal lesion of low signal intensity in the right proximal tibia, with surrounding low-signal-intensity edema.
T1-weighted sagittal magnetic resonance image in a 16-year-old boy with lower leg pain. This image demonstrates a focal lesion of low signal intensity in the right proximal tibia, with surrounding low-signal-intensity edema.
 T1-weighted magnetic resonance image of the shoulder in a 39-year-old woman. This image reveals a lesion of low signal intensity in the right proximal humerus. Note the extension of the predominantly metaphyseal tumor into the epiphysis. The pathologic specimen demonstrated findings that were consistent with aggressive osteoblastoma.
T1-weighted magnetic resonance image of the shoulder in a 39-year-old woman. This image reveals a lesion of low signal intensity in the right proximal humerus. Note the extension of the predominantly metaphyseal tumor into the epiphysis. The pathologic specimen demonstrated findings that were consistent with aggressive osteoblastoma.
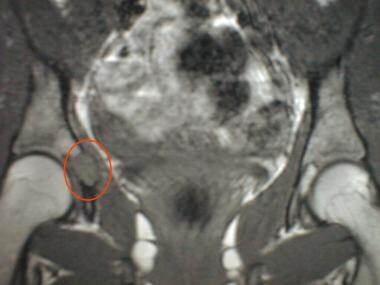 T1-weighted coronal magnetic resonance image through the pelvis in a 14-year-old girl. In this image, the lesion is hypointense compared with the adjacent bone marrow.
T1-weighted coronal magnetic resonance image through the pelvis in a 14-year-old girl. In this image, the lesion is hypointense compared with the adjacent bone marrow.
In the authors' experience, the signal intensity of osteoblastomas on T2-weighted images is variable. Although, in general, the tumors are hyperintense relative to marrow on T2-weighted images, osteoblastomas may be heterogeneous with low signal intensity components on non–fat-suppressed T2-weighted images, presumably reflecting the ossific matrix of the lesion.
(See the images below.)
 T2-weighted magnetic resonance image (MRI) of the left foot. This image demonstrates high signal intensity; the characteristics of this lesion are typical of a neoplastic process, but no specific finding suggests the diagnosis of an osteoblastoma. MRI clearly delineates the extent of the disease process.
T2-weighted magnetic resonance image (MRI) of the left foot. This image demonstrates high signal intensity; the characteristics of this lesion are typical of a neoplastic process, but no specific finding suggests the diagnosis of an osteoblastoma. MRI clearly delineates the extent of the disease process.
 T2-weighted coronal magnetic resonance image of the shoulder in a 39-year-old woman. The tumor demonstrates heterogeneous signal intensity.
T2-weighted coronal magnetic resonance image of the shoulder in a 39-year-old woman. The tumor demonstrates heterogeneous signal intensity.
Adjacent cortical thickening may be demonstrated. MRI often reveals inflammatory edema-type changes in the adjacent marrow and soft tissues, which are particularly evident on fat-suppressed T2-weighted sequences.
(See the images below.)
 T1-weighted magnetic resonance image in a 14-year-old boy. The lesion demonstrates low signal intensity in this image.
T1-weighted magnetic resonance image in a 14-year-old boy. The lesion demonstrates low signal intensity in this image.
 Fat-suppressed T2-weighted magnetic resonance image in a 14-year-old boy. The lesion is hyperintense in this image. Note the surrounding bone marrow edema, depicted with high signal intensity.
Fat-suppressed T2-weighted magnetic resonance image in a 14-year-old boy. The lesion is hyperintense in this image. Note the surrounding bone marrow edema, depicted with high signal intensity.
 T2-weighted coronal magnetic resonance image with fat saturation performed on the knee of a 16-year-old male. This image emphasizes the presence of edema in the adjacent marrow.
T2-weighted coronal magnetic resonance image with fat saturation performed on the knee of a 16-year-old male. This image emphasizes the presence of edema in the adjacent marrow.
 T2-weighted sagittal magnetic resonance image of the spine in a 10-year-old boy. This image delineates the extent of the mass and reveals a homogeneous high signal intensity in the surrounding soft tissues, which is consistent with edema.
T2-weighted sagittal magnetic resonance image of the spine in a 10-year-old boy. This image delineates the extent of the mass and reveals a homogeneous high signal intensity in the surrounding soft tissues, which is consistent with edema.
Both the mass and the inflammatory reaction may enhance after the intravenous administration of gadolinium-based contrast material (see the images below).
T1-weighted gadolinium-enhanced sagittal magnetic resonance image of the spine in a 10-year-old boy. This image reveals contrast enhancement of a mass that is occupying the posterior elements of the C3 vertebra.
 Gadolinium-enhanced magnetic resonance image in a 14-year-old boy. This image demonstrates enhancement in the lesion.
Gadolinium-enhanced magnetic resonance image in a 14-year-old boy. This image demonstrates enhancement in the lesion.
 T1-weighted coronal gadolinium-enhanced magnetic resonance image. This image demonstrates a lesion that enhances slightly, as can be seen in cases with osteoblastomas.
T1-weighted coronal gadolinium-enhanced magnetic resonance image. This image demonstrates a lesion that enhances slightly, as can be seen in cases with osteoblastomas.
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
Nuclear Imaging
Although osteoblastomas accumulate radionuclide on bone scintigraphy studies (see the images below), the scintigraphic appearance of the tumors is nonspecific. Osteoblastomas have a nonspecific increased uptake of bone-seeking agents. This finding adds little to increase the degree of confidence in bone scanning for the diagnosis. Various lesions, such as fractures, osteomyelitis, and other bone tumors, similarly accumulate radionuclide at the site of the lesion as osteoblastomas.
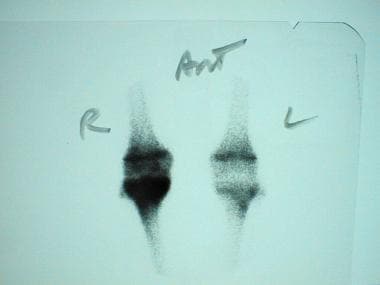 Bone scan in a 16-year-old boy complaining of pain. This image demonstrates increased radiotracer activity in the right proximal tibia that corresponds to the site of the lesion. The increased uptake in the right distal femur is likely due to tumor-associated relative hyperperfusion of the right knee.
Bone scan in a 16-year-old boy complaining of pain. This image demonstrates increased radiotracer activity in the right proximal tibia that corresponds to the site of the lesion. The increased uptake in the right distal femur is likely due to tumor-associated relative hyperperfusion of the right knee.
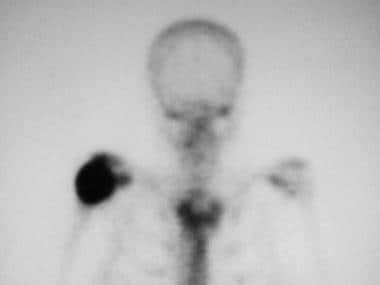 Bone scan in a 39-year-old woman. This image demonstrates abnormal radiotracer accumulation.
Bone scan in a 39-year-old woman. This image demonstrates abnormal radiotracer accumulation.
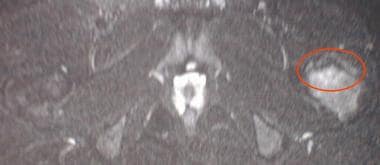
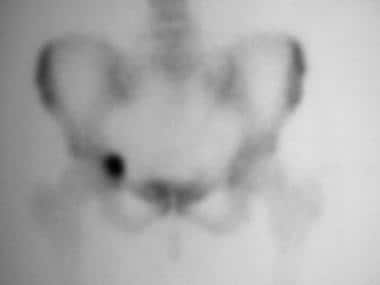 Bone scan in a 14-year-old girl. This image reveals radiotracer accumulation in the patient's right hip.
Bone scan in a 14-year-old girl. This image reveals radiotracer accumulation in the patient's right hip.
-
Lateral radiograph of the cervical spine in a 10-year-old boy. The spinous process of the C3 vertebra is expanded by a mass with ossific matrix.
-
T1-weighted sagittal magnetic resonance image of the spine in a 10-year-old boy. This image suggests the presence of a mass that involves the posterior elements of the C3 vertebra.
-
T1-weighted gadolinium-enhanced sagittal magnetic resonance image of the spine in a 10-year-old boy. This image reveals contrast enhancement of a mass that is occupying the posterior elements of the C3 vertebra.
-
T2-weighted sagittal magnetic resonance image of the spine in a 10-year-old boy. This image delineates the extent of the mass and reveals a homogeneous high signal intensity in the surrounding soft tissues, which is consistent with edema.
-
Computed tomography scan of the cervical spine in a 10-year-old boy. This image reveals a lytic lesion that involves the posterior elements of the C3 vertebra. Cortical expansion of the spinous process and an ossified matrix are noted; these findings are typical and classic findings in cases of osteoblastomas.
-
Knee radiograph from a 16-year-old boy with lower leg pain. This image reveals a somewhat poorly defined and nonspecific lucent lesion in the proximal tibial metaphysis.
-
Bone scan in a 16-year-old boy complaining of pain. This image demonstrates increased radiotracer activity in the right proximal tibia that corresponds to the site of the lesion. The increased uptake in the right distal femur is likely due to tumor-associated relative hyperperfusion of the right knee.
-
T1-weighted sagittal magnetic resonance image in a 16-year-old boy with lower leg pain. This image demonstrates a focal lesion of low signal intensity in the right proximal tibia, with surrounding low-signal-intensity edema.
-
T2-weighted coronal magnetic resonance image with fat saturation performed on the knee of a 16-year-old male. This image emphasizes the presence of edema in the adjacent marrow.
-
Radiograph of the left hip in a 14-year-old boy. This image demonstrates a lytic lesion in the intertrochanteric region of the left femur with a faint, diffuse, surrounding sclerosis. The long bones are the second most common location for osteoblastomas.
-
Computed tomography scan of the left proximal femur in a 14-year-old boy. This image reveals a cortically based nidus with surrounding thickened bone.
-
T1-weighted magnetic resonance image in a 14-year-old boy. The lesion demonstrates low signal intensity in this image.
-
Gadolinium-enhanced magnetic resonance image in a 14-year-old boy. This image demonstrates enhancement in the lesion.
-
Fat-suppressed T2-weighted magnetic resonance image in a 14-year-old boy. The lesion is hyperintense in this image. Note the surrounding bone marrow edema, depicted with high signal intensity.
-
Radiograph of the right shoulder in a 39-year-old woman. This image reveals a large lytic lesion arising in the proximal part of the humerus.
-
Bone scan in a 39-year-old woman. This image demonstrates abnormal radiotracer accumulation.
-
Computed tomography scan in a 39-year-old woman. This image demonstrates faint matrix mineralization.
-
T1-weighted magnetic resonance image of the shoulder in a 39-year-old woman. This image reveals a lesion of low signal intensity in the right proximal humerus. Note the extension of the predominantly metaphyseal tumor into the epiphysis. The pathologic specimen demonstrated findings that were consistent with aggressive osteoblastoma.
-
T2-weighted coronal magnetic resonance image of the shoulder in a 39-year-old woman. The tumor demonstrates heterogeneous signal intensity.
-
Oblique view of the ankle. This radiograph reveals a lucent lesion within the talus, an uncommon location for osteoblastomas. Although this appearance is consistent for an osteoblastoma, it is nonspecific.
-
Lateral radiograph of the ankle.
-
The computed tomography scan findings are nonspecific and have a benign appearance in this image.
-
T1-weighted sagittal magnetic resonance image of the left foot. This image reveals a lesion with low signal intensity in the talus.
-
T2-weighted magnetic resonance image (MRI) of the left foot. This image demonstrates high signal intensity; the characteristics of this lesion are typical of a neoplastic process, but no specific finding suggests the diagnosis of an osteoblastoma. MRI clearly delineates the extent of the disease process.
-
Anteroposterior radiographic view of the pelvis in a 14-year-old girl who presented with right hip pain. This image reveals a lucent, slightly expansile lesion in the acetabulum.
-
Magnified radiographic view of the pelvis in a 14-year-old girl who presented with right hip pain. This image reveals the same lucent, slightly expansile lesion in the acetabulum.
-
Bone scan in a 14-year-old girl. This image reveals radiotracer accumulation in the patient's right hip.
-
Axial computed tomography scan of the right hip in a 14-year-old girl. This image reveals small amounts of matrix mineralization and cortical expansion.
-
T1-weighted coronal magnetic resonance image through the pelvis in a 14-year-old girl. In this image, the lesion is hypointense compared with the adjacent bone marrow.
-
T1-weighted coronal gadolinium-enhanced magnetic resonance image. This image demonstrates a lesion that enhances slightly, as can be seen in cases with osteoblastomas.
-
Axial computed tomography scan that was obtained through the tibial diaphysis. This image demonstrates how an osteoblastoma can resemble a large osteoid osteoma, with the typical radiographic features of a central nidus and surrounding reactive bone.






