Practice Essentials
Liposarcoma is a malignant tumor of mesenchymal origin in which the bulk of the tumor differentiates into adipose tissue. Liposarcoma is a common neoplasm of the soft tissues and affects middle-aged patients. Commonly affected sites include the thigh, gluteal region, retroperitoneum, leg, and shoulder area. Liposarcomas rarely arise from a preexisting lipoma. The clinical presentation depends on the site of the tumors, most of which are palpable masses. [1, 2, 3, 4, 5, 6]
Liposarcomas and lipomas may present with similar symptomatology, as well as similar clinical and imaging findings. Only approximately 15% of soft-tissue sarcomas are liposarcomas, and liposarcomas represent less than 1% of all malignant tumors. [1, 2, 3, 4]
In general, the more aggressive tumors demonstrate more radiopacity, whereas well-differentiated tumors have a greater fat content. Liposarcomas are the most radiosensitive soft-tissue tumors.
Well-differentiated tumors are easily characterized as fat-containing masses, although differentiation between a malignant tumor and a benign one may not be possible. Poorly differentiated tumors may be indistinguishable from other mesothelial tumors, lymphomas, metastases, and inflammatory masses.
Preferred examination
Computed tomography (CT) scanning plays an important role in the preoperative evaluation of lipomatous and myxoid tumors of the soft tissue. [7] Besides providing valuable morphologic information, CT scan findings help differente between various types of lipomatous tumors. Well-differentiated liposarcomas may be distinguished from other types of tumors on the basis of their largely lipomatous appearance. [5] Malignant fibrous histiocytoma, leiomyosarcoma, and desmoid tumors may have a CT scan appearance that is indistinguishable from that of liposarcoma, particularly liposarcoma of the myxoid, mixed myxoid and round cell, round cell, or pleomorphic type.
Gadolinium-enhanced magnetic resonance imaging (MRI) is important in differentiating myxoid liposarcomas from benign cystic tumors. In an MRI study of patients with high-grade myxoid liposarcomas, all high-grade lesions had lipid signal, a peritumoral capsule, and pertumoral contrast enhancement. The strongest indicator was a size of 10 cm or more. [8, 9] Because myxoid tissue is present in many benign and malignant tumors, MRI may not enable a specific diagnosis of a liposarcoma. Moreover, any lesion consisting of edema, an extracellular matrix with a high level of mucopolysaccharide, hyaline cartilage content, and necrosis may appear cystic on MRI scans. [10, 11]
Findings on plain radiographs are nonspecific, and the modality usually offers little except perhaps aid in confirming the presence of a soft-tissue mass. Frequently, fat is not detectable radiologically. Ultrasonography is helpful in confirming the presence of a mass when doubt exists. The use of radionuclides has been anecdotal, but imaging with fluorine-18 fluorodeoxyglucose (18F-FDG) positron emission tomography (PET) scanning holds promise. [12, 13]
(The radiologic characteristics of liposarcomas are demonstrated in the images below.)
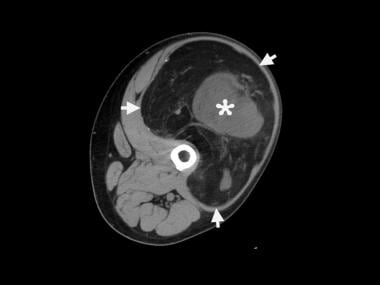 Computed tomography (CT) scan of a left thigh shows a huge mass (arrows) with predominant fat attenuation. The central soft-tissue component (asterisk) and thick, internal septations are consistent with liposarcoma.
Computed tomography (CT) scan of a left thigh shows a huge mass (arrows) with predominant fat attenuation. The central soft-tissue component (asterisk) and thick, internal septations are consistent with liposarcoma.
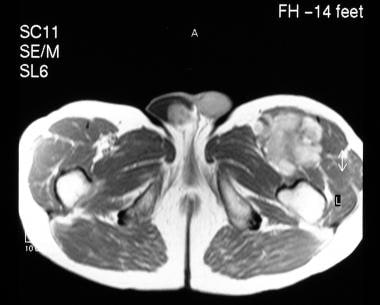
 A 67-year-old man presented with a slowly growing mass on the left side of his groin and with mild left leg claudication. The patient was a nonsmoker and was not diabetic. T1-weighted, coronal magnetic resonance imaging (MRI) shows a 5-cm, low–signal-intensity, lobulated mass in the left upper thigh.
A 67-year-old man presented with a slowly growing mass on the left side of his groin and with mild left leg claudication. The patient was a nonsmoker and was not diabetic. T1-weighted, coronal magnetic resonance imaging (MRI) shows a 5-cm, low–signal-intensity, lobulated mass in the left upper thigh.
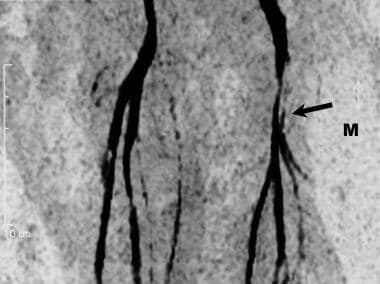 Magnetic resonance (MR) angiogram of the leg vessels in a 67-year-old man who presented with a slowly growing mass on the left side of his groin and with mild left leg claudication. The image shows medial displacement and compression of the left femoral artery, superficial femoral artery, and profunda by the tumor, which resulted in the claudication.
Magnetic resonance (MR) angiogram of the leg vessels in a 67-year-old man who presented with a slowly growing mass on the left side of his groin and with mild left leg claudication. The image shows medial displacement and compression of the left femoral artery, superficial femoral artery, and profunda by the tumor, which resulted in the claudication.
Radiography
The sensitivity and specificity of radiographs are low for liposarcomas. Inflammatory masses and other types of benign and malignant tumors can have a similar appearance. Radiographic findings are seldom diagnostic, and the images may demonstrate a nonspecific soft-tissue mass. Frequently, no fat is detectable. Rarely, calcification (seen in the image below) is present.
Abdominal radiographs in patients with retroperitoneal tumors may reveal a soft-tissue–displacing, gas-filled structure and effacement of the normal fat planes. Contrast-enhanced studies of the gastrointestinal tract may show displacement of the stomach, small bowel, or colon, depending on the location of the tumor.
Intravenous urography may show renal or ureteric displacement; rarely, hydronephrosis is demonstrated.
 A plain radiograph of a left femur demonstrates a large, soft-tissue mass projected over the medial aspect of the thigh (arrowheads). Small areas of radiolucency (asterisk) and calcification (arrow) are shown.
A plain radiograph of a left femur demonstrates a large, soft-tissue mass projected over the medial aspect of the thigh (arrowheads). Small areas of radiolucency (asterisk) and calcification (arrow) are shown.
Computed Tomography
CT scans demonstrate 3 distinct patterns in liposarcomas, as follows:
-
An enhancing, solid, inhomogeneous, poorly defined, infiltrating mass
-
A mixed-pattern tumor with foci of fat interspersed in high-attenuating tissue
-
A pseudocystic water-density tumor.
CT scanning plays an important role in the preoperative evaluation of lipomatous and myxoid tumors of the soft tissue. [14, 15] Besides providing valuable morphologic information, CT scanning helps differentiate between various types of lipomatous tumors. [16, 17] CT scanning is useful in the determination of the tumoral response to radiation therapy or chemotherapy; it is also invaluable in the detection of tumor recurrence. Malignant fibrous histiocytoma, leiomyosarcoma, and desmoid tumors may have an appearance that is indistinguishable from that of liposarcoma, particularly liposarcoma of the myxoid, mixed myxoid and round cell, round cell, or pleomorphic type.
Liposarcomas of the myxoid type, the mixed myxoid and round cell type, the round cell type, and the pleomorphic type are usually poorly defined, with attenuation values of 12-38 HU and varying degrees of contrast enhancement. [18, 19] Calcification is detectable in as many as 12% of the tumors.
Occasionally, the mass may appear inhomogeneous, with areas of low-attenuating, fatty components. [20, 21] Fatty components may be demonstrated better with planar tomography.
(The CT-scan characteristics of liposarcomas are demonstrated below.)
Computed tomography (CT) scan of a left thigh shows a huge mass (arrows) with predominant fat attenuation. The central soft-tissue component (asterisk) and thick, internal septations are consistent with liposarcoma.
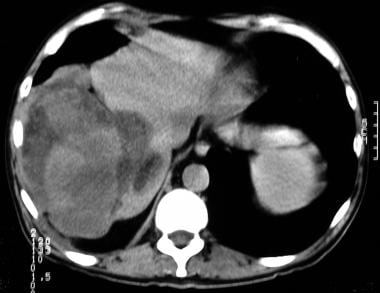 A 50-year-old man presented with a 6-month history of a dull ache over the right hypochondrium. An ultrasonogram (not shown) depicted a poorly defined, infiltrating, echogenic mass in the right hepatic lobe with shadowing. A nonenhanced, axial computed tomography (CT) scan shows a low–fat-attenuating mass under the diaphragm; the mass displaces the liver to the left.
A 50-year-old man presented with a 6-month history of a dull ache over the right hypochondrium. An ultrasonogram (not shown) depicted a poorly defined, infiltrating, echogenic mass in the right hepatic lobe with shadowing. A nonenhanced, axial computed tomography (CT) scan shows a low–fat-attenuating mass under the diaphragm; the mass displaces the liver to the left.
 Contrast-enhanced, axial computed tomography (CT) scan of an abdomen demonstrates a huge, intra-abdominal, fatty mass with a soft-tissue component (arrow) and thick septations. The mass displaces the descending colon and the left kidney posteriorly.
Contrast-enhanced, axial computed tomography (CT) scan of an abdomen demonstrates a huge, intra-abdominal, fatty mass with a soft-tissue component (arrow) and thick septations. The mass displaces the descending colon and the left kidney posteriorly.
Magnetic Resonance Imaging
Most liposarcomas appear well defined on MRI scans, mostly with lobulated margins. [22, 23, 8, 24] Well-differentiated liposarcomas are made up primarily of fat and have septations or nodules; these neoplasms are hyperintense on T2-weighted images. [18, 25, 26] After the administration of contrast material, well-differentiated liposarcomas may enhance minimally or not at all. [10, 11] (See the images below.)
A spectrum of abnormal MRI findings may occur in the myxoid type, depending on the quantity of fat and myxoid material that is present, on the degree of cellularity and vascularity, and on whether or not necrosis exists. [27] Most myxoid tumors have linear or lacy, amorphous foci of fat. [28] Some myxoid tumors may appear cystic on nonenhanced MRI scans, but they are usually enhancing after the administration of contrast agents. [29, 9]
Pleomorphic tumors show a markedly heterogeneous internal structure and moderate contrast enhancement. The malignancy grade is believed to increase in parallel with tumor heterogeneity and contrast enhancement.
A 67-year-old man presented with a slowly growing mass on the left side of his groin and with mild left leg claudication. The patient was a nonsmoker and was not diabetic. T1-weighted, coronal magnetic resonance imaging (MRI) shows a 5-cm, low–signal-intensity, lobulated mass in the left upper thigh.
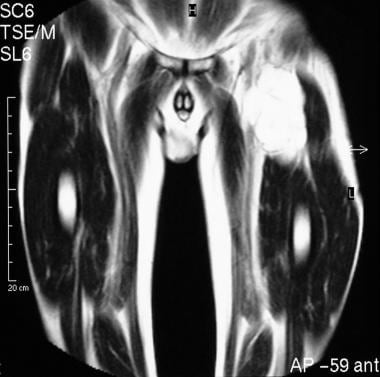 T2-weighted, coronal magnetic resonance imaging (MRI) scan of the left upper thigh in a 67-year-old man who presented with a slowly growing mass on the left side of his groin and with mild left leg claudication. The image shows a high–signal-intensity, lobulated, septate mass in the region of the groin.
T2-weighted, coronal magnetic resonance imaging (MRI) scan of the left upper thigh in a 67-year-old man who presented with a slowly growing mass on the left side of his groin and with mild left leg claudication. The image shows a high–signal-intensity, lobulated, septate mass in the region of the groin.
 Contrast-enhanced, axial magnetic resonance imaging (MRI) scan of the upper thigh in a 67-year-old man who presented with a slowly growing mass on the left side of his groin and with mild left leg claudication. The image shows fairly intense tumor enhancement.
Contrast-enhanced, axial magnetic resonance imaging (MRI) scan of the upper thigh in a 67-year-old man who presented with a slowly growing mass on the left side of his groin and with mild left leg claudication. The image shows fairly intense tumor enhancement.
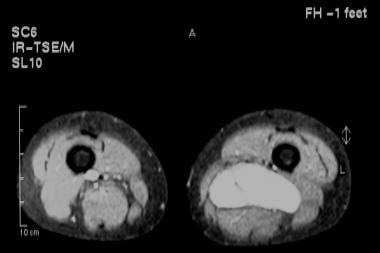
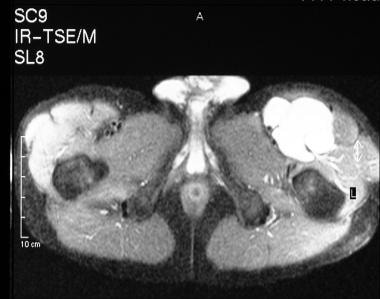 Short-tau inversion recovery, turbo spin-echo, axial magnetic resonance imaging (MRI) scan of the left upper thigh in a 67-year-old man who presented with a slowly growing mass on the left side of his groin and with mild left leg claudication. The image shows fluid signal intensity within the tumor.
Short-tau inversion recovery, turbo spin-echo, axial magnetic resonance imaging (MRI) scan of the left upper thigh in a 67-year-old man who presented with a slowly growing mass on the left side of his groin and with mild left leg claudication. The image shows fluid signal intensity within the tumor.
 Sagittal, T1-weighted magnetic resonance imaging (MRI) scan in a 32-year-old woman presenting with a palpable mass above the left popliteal fossa. The image shows a low–signal-intensity, lobulated mass in the region of the Hunter canal.
Sagittal, T1-weighted magnetic resonance imaging (MRI) scan in a 32-year-old woman presenting with a palpable mass above the left popliteal fossa. The image shows a low–signal-intensity, lobulated mass in the region of the Hunter canal.
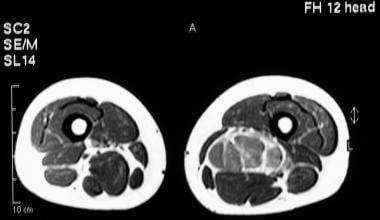 Axial, T1-weighted magnetic resonance imaging (MRI) scan in a 32-year-old woman obtained through a palpable mass above the left popliteal fossa. The image shows a low–signal-intensity, lobulated mass.
Axial, T1-weighted magnetic resonance imaging (MRI) scan in a 32-year-old woman obtained through a palpable mass above the left popliteal fossa. The image shows a low–signal-intensity, lobulated mass.
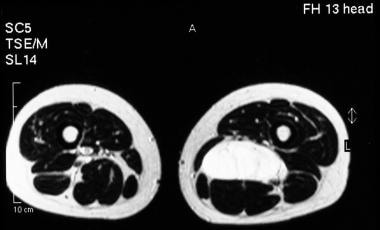 Axial, T2-weighted magnetic resonance imaging (MRI) scan in a 32-year-old woman presenting with a palpable mass above the left popliteal fossa. The image shows a high–signal-intensity, lobulated mass.
Axial, T2-weighted magnetic resonance imaging (MRI) scan in a 32-year-old woman presenting with a palpable mass above the left popliteal fossa. The image shows a high–signal-intensity, lobulated mass.
 Fat-saturated magnetic resonance imaging (MRI) scan through the tumor in a 32-year-old woman presenting with a palpable mass above the left popliteal fossa. The image shows fluid signal intensity within the mass.
Fat-saturated magnetic resonance imaging (MRI) scan through the tumor in a 32-year-old woman presenting with a palpable mass above the left popliteal fossa. The image shows fluid signal intensity within the mass.
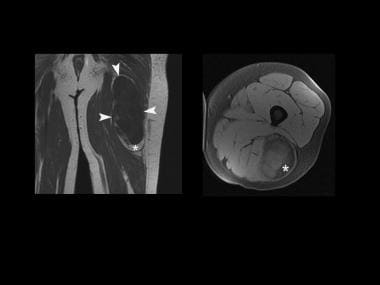 Magnetic resonance imaging (MRI) scans (coronal, T1-weighted image and axial, T1-weighted image with fat saturation) show a soft-tissue mass of the posterior aspect of a thigh. It has a predominantly low T1 signal intensity except in its inferior portion, which has a high T1 signal intensity isointense to subcutaneous fat. Complete suppression is shown on the axial, T1-weighted image with fat saturation (asterisk).
Magnetic resonance imaging (MRI) scans (coronal, T1-weighted image and axial, T1-weighted image with fat saturation) show a soft-tissue mass of the posterior aspect of a thigh. It has a predominantly low T1 signal intensity except in its inferior portion, which has a high T1 signal intensity isointense to subcutaneous fat. Complete suppression is shown on the axial, T1-weighted image with fat saturation (asterisk).
Well-differentiated liposarcomas may be distinguished from other types of tumors on the basis of their largely lipomatous appearance. [30, 31] Gadolinium-enhanced imaging is important in differentiating myxoid liposarcomas from benign cystic tumors.
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). For more information, see Nephrogenic Systemic Fibrosis. The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or magnetic resonance angiography (MRA) scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness. For more information, see Medscape.
Myxoid tissue is present in many benign and malignant tumors, including extraskeletal myxoid chondrosarcomas, intramuscular myxomas, ganglia, and myxoid, malignant fibrous histiocytomas, in addition to myxoid liposarcomas. Any lesion consisting of edema, an extracellular matrix with a high level of mucopolysaccharide, hyaline cartilage content, and necrosis may appear cystic on MRI scans.
Ultrasonography
Ultrasonography is helpful in confirming the presence of a mass. [32, 33] Liposarcomas are usually hyperechoic. Retroperitoneal liposarcomas are highly reflective, although this feature may be absent when the tumor is poorly differentiated.
The finding of a solid retroperitoneal mass that demonstrates a heterogeneous echo pattern with an echo-poor center usually suggests a sarcoma. The central echo-poor area is usually the result of hemorrhage or necrosis (because the tumors tend to outgrow their blood supply).
A well-differentiated, peripheral liposarcoma is usually hyperechoic and may be indistinguishable from a lipoma; however, Doppler ultrasonography studies reveal that a liposarcoma is more vascular than a lipoma. [34]
The remaining 3 varieties of liposarcoma appear as a heterogeneous soft-tissue mass with no distinguishing characteristics.
Confirming the retroperitoneal origin of a tumor is not always possible with ultrasonography. However, some characteristic features may be helpful in locating the tumor's origin. These include anterior displacement of the pancreas, abdominal aorta, inferior vena cava, kidneys, and ascending or descending colon. The benign or malignant nature of retroperitoneal tumors cannot be determined by using ultrasonography.
Vascular tumors, such as hemangiopericytomas, can be highly reflective, presumably because of the numerous tissue interfaces with multiple vascular walls. Distinguishing poorly differentiated liposarcomas from other types of retroperitoneal or peripheral masses is not always possible. A peripheral, well-differentiated liposarcoma may have the appearance of a lipoma.
Nuclear Imaging
It appears that gallium-67 (67Ga) scanning can play an important part in the evaluation of patients presenting with a primary or metastatic soft-tissue sarcoma, according to a study by Imaeda et al. In the investigation, 67Ga citrate scintigraphy scanning was evaluated in 90 patients with soft-tissue tumors of the limbs. Positive findings were found in 78% of patients with malignant tumors, 25% of patients with benign lesions, and 31% of patients with other types of lesions. Distinguishing liposarcoma from lipoma appeared to be possible by means of a 67Ga scan, according to the authors. [35]
Gallium-67 scanning may also have a role in imaging liposarcoma recurrence. [36]
A study of 78 patients with malignant soft-tissue sarcoma who were evaluated with thallium-201 (201Tl) chloride revealed a radionuclide sensitivity of 81%. [37] Another study showed that technetium-99m (99mTc) pertechnetate can potentially aid in the localization of malignant soft-tissue tumors and may be useful in their evaluation. [38, 39] Another study demonstrated that 99mTc bleomycin and 99mTc pentavalent dimercaptosuccinic acid (99mTc[V]-DMSA) scanning can better localize liposarcomas than 67Ga imaging. [40]
Vertebral metastases from a myxoid liposarcoma may not show radionuclide uptake on isotope bone scans and fluorodeoxyglucose positron emission tomography (FDG-PET) scanning, even when extraskeletal extensions are present. Similarly, even a fractured vertebra may not always be visible on FDG-PET scans. [41]
Angiography
Angiography may be useful for preoperative planning, intra-arterial infusion, and/or transcatheter embolization. Liposarcomas are usually hypovascular to moderately vascular, and they displace major vessels, particularly the inferior vena cava. [42] Moderately hypervascular liposarcomas may show irregular, fine tumor vessels and areas of tumor stain (as shown in the images below). Venous filling may occur early, and the veins may be dilated and tortuous. Displacement of the kidneys and arteries is seen in all except very small retroperitoneal tumors.
Angiography cannot help in the differentiation of liposarcomas from other types of sarcomas. Benign and malignant retroperitoneal tumors can be avascular.
 Moderately hypervascular tumor in the right upper thigh shows irregular, fine tumor vessels and areas of tumor stain.
Moderately hypervascular tumor in the right upper thigh shows irregular, fine tumor vessels and areas of tumor stain.
 Moderately hypervascular tumor in the right upper thigh shows irregular, fine tumor vessels and areas of tumor stain.
Moderately hypervascular tumor in the right upper thigh shows irregular, fine tumor vessels and areas of tumor stain.
Questions & Answers
Overview
What are the preferred modalities for liposarcoma imaging?
What are limitations of liposarcoma imaging?
Which radiography findings are characteristic of liposarcoma?
Which findings on CT scans are characteristic of liposarcoma?
What is the degree of confidence for CT scanning of liposarcoma?
Which conditions may create false positive or negative findings on CT scans of liposarcomas?
Which MRI findings are characteristic of liposarcoma?
What is the degree of confidence for MRI of liposarcoma?
Which conditions may create false positive or negative findings on MRIs of liposarcomas?
What is the role of ultrasonography in liposarcoma imaging?
What is the degree of confidence for ultrasonography of liposarcoma?
Which conditions may create false positive or negative findings on ultrasonography of liposarcomas?
What is the role of nuclear imaging in liposarcoma imaging?
What is the role of angiography in liposarcoma imaging?
-
Computed tomography (CT) scan of a left thigh shows a huge mass (arrows) with predominant fat attenuation. The central soft-tissue component (asterisk) and thick, internal septations are consistent with liposarcoma.
-
A 67-year-old man presented with a slowly growing mass on the left side of his groin and with mild left leg claudication. The patient was a nonsmoker and was not diabetic. T1-weighted, coronal magnetic resonance imaging (MRI) shows a 5-cm, low–signal-intensity, lobulated mass in the left upper thigh.
-
T2-weighted, coronal magnetic resonance imaging (MRI) scan of the left upper thigh in a 67-year-old man who presented with a slowly growing mass on the left side of his groin and with mild left leg claudication. The image shows a high–signal-intensity, lobulated, septate mass in the region of the groin.
-
Contrast-enhanced, axial magnetic resonance imaging (MRI) scan of the upper thigh in a 67-year-old man who presented with a slowly growing mass on the left side of his groin and with mild left leg claudication. The image shows fairly intense tumor enhancement.
-
Short-tau inversion recovery, turbo spin-echo, axial magnetic resonance imaging (MRI) scan of the left upper thigh in a 67-year-old man who presented with a slowly growing mass on the left side of his groin and with mild left leg claudication. The image shows fluid signal intensity within the tumor.
-
Magnetic resonance (MR) angiogram of the leg vessels in a 67-year-old man who presented with a slowly growing mass on the left side of his groin and with mild left leg claudication. The image shows medial displacement and compression of the left femoral artery, superficial femoral artery, and profunda by the tumor, which resulted in the claudication.
-
Moderately hypervascular tumor in the right upper thigh shows irregular, fine tumor vessels and areas of tumor stain.
-
Moderately hypervascular tumor in the right upper thigh shows irregular, fine tumor vessels and areas of tumor stain.
-
Sagittal, T1-weighted magnetic resonance imaging (MRI) scan in a 32-year-old woman presenting with a palpable mass above the left popliteal fossa. The image shows a low–signal-intensity, lobulated mass in the region of the Hunter canal.
-
Axial, T1-weighted magnetic resonance imaging (MRI) scan in a 32-year-old woman obtained through a palpable mass above the left popliteal fossa. The image shows a low–signal-intensity, lobulated mass.
-
Axial, T2-weighted magnetic resonance imaging (MRI) scan in a 32-year-old woman presenting with a palpable mass above the left popliteal fossa. The image shows a high–signal-intensity, lobulated mass.
-
Fat-saturated magnetic resonance imaging (MRI) scan through the tumor in a 32-year-old woman presenting with a palpable mass above the left popliteal fossa. The image shows fluid signal intensity within the mass.
-
Ultrasonogram in a 32-year-old woman with a mass above the left popliteal fossa shows a hypoechoic (but solid) mass.
-
A 50-year-old man presented with a 6-month history of a dull ache over the right hypochondrium. An ultrasonogram (not shown) depicted a poorly defined, infiltrating, echogenic mass in the right hepatic lobe with shadowing. A nonenhanced, axial computed tomography (CT) scan shows a low–fat-attenuating mass under the diaphragm; the mass displaces the liver to the left.
-
Hepatic angiogram in a 50-year-old man who presented with a 6-month history of a dull ache over the right hypochondrium. The image shows a hypovascular mass that displaces the liver medially. The mass was believed to represent a retroperitoneal liposarcoma; however, at laparotomy, the tumor was discovered to be intrahepatic. The histologic appearance was that of a high-grade liposarcoma infiltrating the diaphragm.
-
A plain radiograph of a left femur demonstrates a large, soft-tissue mass projected over the medial aspect of the thigh (arrowheads). Small areas of radiolucency (asterisk) and calcification (arrow) are shown.
-
Magnetic resonance imaging (MRI) scans (coronal, T1-weighted image and axial, T1-weighted image with fat saturation) show a soft-tissue mass of the posterior aspect of a thigh. It has a predominantly low T1 signal intensity except in its inferior portion, which has a high T1 signal intensity isointense to subcutaneous fat. Complete suppression is shown on the axial, T1-weighted image with fat saturation (asterisk).
-
Contrast-enhanced, axial computed tomography (CT) scan of an abdomen demonstrates a huge, intra-abdominal, fatty mass with a soft-tissue component (arrow) and thick septations. The mass displaces the descending colon and the left kidney posteriorly.






