Practice Essentials
A chondroblastoma is a rare benign cartilaginous neoplasm that characteristically arises in the epiphysis of a long bone in young patients. [1, 2, 3, 4] Chondroblastomas account for less than 2% of all bone tumors, and metaphyseal or diaphyseal chondroblastoma occurs in only 2% of all cases of chondroblastoma. [5, 6] Case reports describe occurrences in the temporal bone [7, 8, 9] and thoracic spine. [10, 11, 12]
Most chondroblastomas are diagnosed in the second to third decade of life (mean age, 19-23 yr), with a male predominance. Chondroblastoma of the temporal bone typically occurs in older males (30-40 yr), and patients with tumors that arise from the epiphyseal cartilage of the long bones are generally between 20 and 30 years of age. [1, 7] In one study, by Angelini et al, of 23 patients with chondroblastoma who were older than 30 years (mean, 40 yr; range, 30-59 yr), the tumors involved the small bones (talus, calcaneus, acromion, cuneiform, metatarsals) in 15 patients and the long bones in 8 patients. [13]
Imaging and differential diagnosis
The preferred modalities for evaluation of chondroblastomas are standard radiography and either computed tomography (CT) scanning or magnetic resonance imaging (MRI). [14, 15, 16, 17] Underexposed radiographs may fail to depict a chondroblastoma. CT scanning may be useful for the better definition of possible cortical erosion and matrix mineralization, although this modality is usually inferior to MRI in the evaluation of transphyseal or transcortical extension, both of which are important factors in preoperative planning. Other modalities may be useful on a case-by-case basis.
The differential diagnosis includes chondrosarcoma, skeletal eosinophilic granuloma, giant cell tumor, hemangioma of bone, and osteomyelitis. Other considerations are degenerative cysts of osteoarthritis (eg, subchondral cysts, geodes), intraosseous ganglion, and avascular necrosis. Chondroblastoma-like osteosarcoma is a very rare subtype of osteoscarcoma that may be confused with chondroblastoma. [18]
Although a chondroblastoma has nonspecific findings, if any, at physical examination, the imaging findings of chondroblastomas are often straightforward when a nonaggressive epiphyseal lesion is identified in a child or adolescent patient. From an imaging standpoint, pitfalls reflect a lack of detection of the lesion or a misinterpretation of the radiologic findings.
Occasionally, a chondroblastoma may be mistaken for other entities listed in the differential diagnosis (see above), but these other entities are almost never confined to the epiphysis, with the exception of degenerative cysts, avascular necrosis, and clear cell chondrosarcomas (which usually occur in older patients), and infection (which usually occurs in patients with fever, leukocytosis, and an elevated erythrocyte sedimentation rate [ESR]).
Confusion may arise if the chondroblastoma extends across the physis and mimics a metaphyseal lesion or if it arises in an atypical location such as the pelvis. If the chondroblastoma crosses the physis, it may be mistaken for either a chondromyxoid fibroma or a giant cell tumor (which typically occurs in a slightly older patient population, generally has no mineralization, and usually has nonsclerotic borders). If the chondroblastoma occurs in the pelvis, it may mimic either fibrous dysplasia or a nonossifying fibroma, both of which are often multifocal "don't touch" lesions.
Angiography may be used to create a vascular road map of the chondroblastoma for surgical planning, but the angiograms usually show no vascular abnormality. A periosteal reaction and neovascularity at the cortical surface near the tumor site or in the adjacent synovium have been described. Vascular displacement may be present if the tumor is large.
(The following 4 images are from the same patient with chondroblastoma.)
 Plain radiograph of the distal femoral epiphysis in a 12-year-old boy. This image shows a chondroblastoma with a characteristically lucent lesion and well-defined margins. Extension across the physis was confirmed with computed tomography scanning and magnetic resonance imaging.
Plain radiograph of the distal femoral epiphysis in a 12-year-old boy. This image shows a chondroblastoma with a characteristically lucent lesion and well-defined margins. Extension across the physis was confirmed with computed tomography scanning and magnetic resonance imaging.
 Coronal reconstructed computed tomography scan of the knee in a 12-year-old boy. This image confirms extension of the chondroblastoma into the metaphysis.
Coronal reconstructed computed tomography scan of the knee in a 12-year-old boy. This image confirms extension of the chondroblastoma into the metaphysis.
 Coronal T1-weighted magnetic resonance image of the knee in a 12-year-old boy. This image also confirms extension of the chondroblastoma into the metaphysis.
Coronal T1-weighted magnetic resonance image of the knee in a 12-year-old boy. This image also confirms extension of the chondroblastoma into the metaphysis.
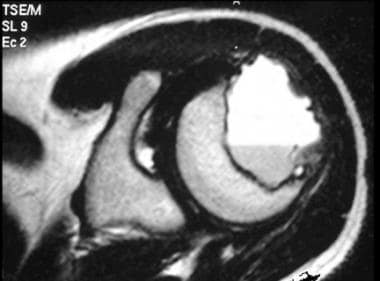
 Sagittal T2-weighted magnetic resonance image of the knee in a 12-year-old boy. This image shows extension of the chondroblastoma across the physis. At histologic examination, central foci of low signal intensity, which are common in chondroblastomas, may be correlated with hypercellularity of the chondroblasts, calcification, and/or hemosiderin deposition.
Sagittal T2-weighted magnetic resonance image of the knee in a 12-year-old boy. This image shows extension of the chondroblastoma across the physis. At histologic examination, central foci of low signal intensity, which are common in chondroblastomas, may be correlated with hypercellularity of the chondroblasts, calcification, and/or hemosiderin deposition.
Anatomy
Chondroblastomas typically occur in the epiphysis or apophysis of a long tubular bone, and the tumor is confined to the epiphysis in 40% of cases. In the remainder of the cases, the tumor extends to the adjacent metaphysis. Rarely, chondroblastomas arise in the metaphysis and, even less frequently, in the diaphysis.
The most commonly affected site is the lower extremity (72% of cases), in which 50% of the chondroblastomas occur around the knee (see the following images).
Plain radiograph of the distal femoral epiphysis in a 12-year-old boy. This image shows a chondroblastoma with a characteristically lucent lesion and well-defined margins. Extension across the physis was confirmed with computed tomography scanning and magnetic resonance imaging.
 Plain radiograph of the proximal tibia in a 14-year-old boy. This image demonstrates a chondroblastoma that has well-circumscribed, thin, sclerotic margins. Chondroblastomas may have sclerotic, nonsclerotic, or incompletely sclerotic borders.
Plain radiograph of the proximal tibia in a 14-year-old boy. This image demonstrates a chondroblastoma that has well-circumscribed, thin, sclerotic margins. Chondroblastomas may have sclerotic, nonsclerotic, or incompletely sclerotic borders.
The femur is involved in 33% of cases; the humerus, in 20%; and the tibia, in 18%. [19] Lesions in the proximal femur are 3 times more likely to occur in the greater trochanter than in the femoral head (see the image below).
 Plain radiograph of the greater trochanter in a 24-year-old man. Chondroblastomas that occur in the proximal femur are 3 times more likely to occur in the greater trochanter than in the femoral head.
Plain radiograph of the greater trochanter in a 24-year-old man. Chondroblastomas that occur in the proximal femur are 3 times more likely to occur in the greater trochanter than in the femoral head.
About 90% of the lesions in the humerus occur in the proximal humeral head (see the following image).
 Plain radiograph of the right upper extremity of a 16-year-old girl. This image shows a chondroblastoma in the humeral head.
Plain radiograph of the right upper extremity of a 16-year-old girl. This image shows a chondroblastoma in the humeral head.
Approximately 10% of all chondroblastomas occur in the small bones of the hands and feet; the talus and calcaneus are common sites (see the following image).
 Plain radiograph of the talus in a 12-year-old boy. About 10% of all chondroblastomas occur in the small bones of the hands and feet. The talus and calcaneus are relatively common sites.
Plain radiograph of the talus in a 12-year-old boy. About 10% of all chondroblastomas occur in the small bones of the hands and feet. The talus and calcaneus are relatively common sites.
Other rare sites include the para-acetabular innominate bone, ribs, skull, mandible, maxillae, vertebrae, scapulae, patellae [20] , and sternum (see the images below)
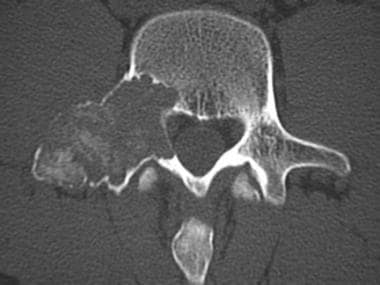
 Plain radiograph of the pedicle and transverse process of a lumbar vertebra. Although the diagnosis of osteoblastoma was made on the basis of the radiographic appearance of the tumor, chondroblastoma was confirmed at pathologic examination.
Plain radiograph of the pedicle and transverse process of a lumbar vertebra. Although the diagnosis of osteoblastoma was made on the basis of the radiographic appearance of the tumor, chondroblastoma was confirmed at pathologic examination.
 Oblique plain radiograph of the patella in a 16-year-old girl. Note the presence of a comminuted pathologic fracture in association with the chondroblastoma.
Oblique plain radiograph of the patella in a 16-year-old girl. Note the presence of a comminuted pathologic fracture in association with the chondroblastoma.
 Plain radiograph of the acromion in a 54-year-old man. The chondroblastoma is in an unusual location and is atypically present in an older patient.
Plain radiograph of the acromion in a 54-year-old man. The chondroblastoma is in an unusual location and is atypically present in an older patient.
Radiologic intervention
Rybak et al demonstrated that radiofrequency ablation can be used safely and effectively to treat selected cases of chondroblastoma. [21] In their study, radiofrequency ablation was performed in 17 patients with a single-tip electrode, using CT for guidance. Of 17 patients, all patients reported relief of symptoms on postprocedure day 1. Of the 14 available for follow-up, 12 had complete relief of symptoms with no need for medications and full return to all activities. The authors noted, however, that larger lesions beneath weight-bearing surfaces should be approached with caution because of an increased risk of articular collapse and recurrence. [21]
Angiographic embolotherapy has no role in cases of chondroblastomas, although image-guided percutaneous therapy for difficult surgical cases may become more common.
Radiography
The radiographic appearance of chondroblastomas is reflected by the benign, slow-growing nature of these lesions. The tumors typically arise in the epiphysis of a long bone, most commonly in the lower extremities. They are usually round or oval, geographic, lucent lesions with sharply marginated borders (see the first image below). The rim may be sclerotic, nonsclerotic, or incompletely sclerotic (see the second image below).
Plain radiograph of the distal femoral epiphysis in a 12-year-old boy. This image shows a chondroblastoma with a characteristically lucent lesion and well-defined margins. Extension across the physis was confirmed with computed tomography scanning and magnetic resonance imaging.
Plain radiograph of the proximal tibia in a 14-year-old boy. This image demonstrates a chondroblastoma that has well-circumscribed, thin, sclerotic margins. Chondroblastomas may have sclerotic, nonsclerotic, or incompletely sclerotic borders.
About 80% of chondroblastomas are 1-4 cm in diameter, although lesions as large as 13 cm have been reported. An eccentric position of the tumor in the epiphysis is most common, but central locations sometimes occur. Approximately 40-50% of chondroblastomas are confined to the epiphysis, with the remainder demonstrating metaphyseal extension, as shown in the first image above and the CT scans and MRI below.
Coronal reconstructed computed tomography scan of the knee in a 12-year-old boy. This image confirms extension of the chondroblastoma into the metaphysis.
Coronal T1-weighted magnetic resonance image of the knee in a 12-year-old boy. This image also confirms extension of the chondroblastoma into the metaphysis.
Sagittal T2-weighted magnetic resonance image of the knee in a 12-year-old boy. This image shows extension of the chondroblastoma across the physis. At histologic examination, central foci of low signal intensity, which are common in chondroblastomas, may be correlated with hypercellularity of the chondroblasts, calcification, and/or hemosiderin deposition.
Chondroblastomas have variable matrix mineralization patterns. About 40% are uniformly lucent, and 60% have a mottled opacity due to amorphous calcification or peripheral septae. The calcifications occur less often in the punctate, "rings and arcs" form. Opacity due to septae and calcification is best differentiated on CT scans.
With increasing size, chondroblastomas may extend into the metaphysis and cause endosteal scalloping, bulging of the overlying cortex, and/or periosteal reaction. Periosteal reaction occurs in 15-30% of cases and may be solid or laminated (see the image below), but it never occurs in the aggressive sunburst or Codman triangle pattern. The longer the lesion is present, the more likely the presence of periosteal reaction and matrix mineralization. Periosteal reaction may be distant from the actual tumor.
 Plain radiograph of the proximal humerus in a 17-year-old boy. A subtle, solid, adjacent metaphyseal periosteal reaction is present medially due to the chondroblastoma. A metaphyseal periosteal reaction occurs in 15-30% of chondroblastomas.
Plain radiograph of the proximal humerus in a 17-year-old boy. A subtle, solid, adjacent metaphyseal periosteal reaction is present medially due to the chondroblastoma. A metaphyseal periosteal reaction occurs in 15-30% of chondroblastomas.
Computed Tomography
CT scanning with a review of the soft-tissue and bone windows is rarely necessary in chondroblastoma. Typically, this modality is reserved for the evaluation of aggressive or recurrent tumors. CT scans can depict matrix mineralization, soft-tissue extension, and cortical erosion, if present. [20] A fluid-fluid level may be identified; this is a nonspecific finding that also occurs with aneurysmal bone cysts, giant cell tumors, and telangiectatic osteosarcoma. [22, 23] Coronal and sagittal reconstructions, like conventional CT scans, can be used to assess extension across the physeal plate. (See the images below.)
Coronal reconstructed computed tomography scan of the knee in a 12-year-old boy. This image confirms extension of the chondroblastoma into the metaphysis.
 Axial computed tomography scan of a humeral head chondroblastoma in a 16-year-old girl. The mottled central opacity that was demonstrated on the plain radiograph was due to amorphous calcifications within the lesion, which occur in approximately 60% of all chondroblastomas.
Axial computed tomography scan of a humeral head chondroblastoma in a 16-year-old girl. The mottled central opacity that was demonstrated on the plain radiograph was due to amorphous calcifications within the lesion, which occur in approximately 60% of all chondroblastomas.
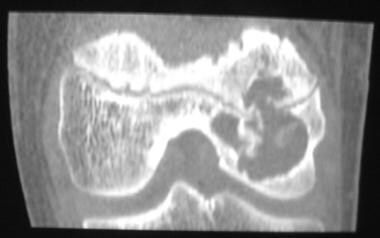
 Axial computed tomography scan of a spinal chondroblastoma. Chondroblastoma rarely occurs in the spine.
Axial computed tomography scan of a spinal chondroblastoma. Chondroblastoma rarely occurs in the spine.
Magnetic Resonance Imaging
MRI provides useful information regarding the extent of the tumor when a chondroblastoma extends to the metaphysis. The signal-intensity characteristics of the chondroblastoma reflect the prominent cellular stroma of the tumor, which has low signal intensity on T1-weighted images and variable signal intensity on T2-weighted images (see the following images). [24]
Coronal T1-weighted magnetic resonance image of the knee in a 12-year-old boy. This image also confirms extension of the chondroblastoma into the metaphysis.
Sagittal T2-weighted magnetic resonance image of the knee in a 12-year-old boy. This image shows extension of the chondroblastoma across the physis. At histologic examination, central foci of low signal intensity, which are common in chondroblastomas, may be correlated with hypercellularity of the chondroblasts, calcification, and/or hemosiderin deposition.
 Coronal T1-weighted magnetic resonance image of a proximal tibial chondroblastoma in a 14-year-old boy.
Coronal T1-weighted magnetic resonance image of a proximal tibial chondroblastoma in a 14-year-old boy.
 Coronal T2-weighted magnetic resonance image (MRI) of a proximal tibial chondroblastoma in a 14-year-old boy. The lesion is confined to the epiphysis. The presence of surrounding edema is best depicted with MRI.
Coronal T2-weighted magnetic resonance image (MRI) of a proximal tibial chondroblastoma in a 14-year-old boy. The lesion is confined to the epiphysis. The presence of surrounding edema is best depicted with MRI.
 Coronal T2-weighted magnetic resonance image of a greater trochanter chondroblastoma in a 24-year-old man.
Coronal T2-weighted magnetic resonance image of a greater trochanter chondroblastoma in a 24-year-old man.
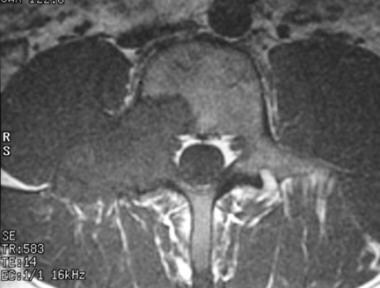 Axial nonenhanced T1-weighted magnetic resonance image of a spinal chondroblastoma.
Axial nonenhanced T1-weighted magnetic resonance image of a spinal chondroblastoma.
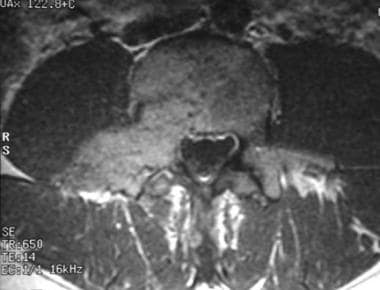 Contrast-enhanced axial T1-weighted magnetic resonance image of a spinal chondroblastoma. This image shows nonspecific but uniform enhancement throughout the lesion.
Contrast-enhanced axial T1-weighted magnetic resonance image of a spinal chondroblastoma. This image shows nonspecific but uniform enhancement throughout the lesion.
Foci of hypointense signals in the lesion on T2-weighted images are purportedly correlated with the histologic findings of abundant immature chondroid matrix, chondroblastic hypercellularity, calcification, and hemosiderin deposition. [24] Occasionally, the hypointensity is uniform throughout the lesion. As with CT scans, MRIs may show fluid-fluid levels (see the image below).
 Axial T2-weighted magnetic resonance image of a humeral head chondroblastoma in a 17-year-old boy. Fluid-fluid levels are occasionally seen on images of chondroblastomas, which can simulate aneurysmal bone cysts.
Axial T2-weighted magnetic resonance image of a humeral head chondroblastoma in a 17-year-old boy. Fluid-fluid levels are occasionally seen on images of chondroblastomas, which can simulate aneurysmal bone cysts.
In contrast to chondroblastomas, the signal intensities of enchondromas, osteochondromas, and well-differentiated osteosarcomas tend to be high on T2-weighted images. Clear cell chondrosarcomas, however, show characteristics similar to those of chondroblastomas, and the signal intensity on T2-weighted images varies with the cellularity of the tumor and the extent of the adjacent inflammatory change.
The adjacent inflammatory changes, not seen with standard radiography or CT scans, are usually hyperintense on T2-weighted MRIs. This adjacent signal-intensity abnormality may be misleading, because its extent is discordant with the radiographic appearance. When such discordance is encountered, the radiographic findings should be the basis for the diagnosis.
Nuclear Imaging
Nuclear medicine studies have limited value in the evaluation of chondroblastomas. Avid uptake of the bone-seeking radiopharmaceutical agent may, in part or in whole, be due to the regional hyperemia of the tumor (see the following image).
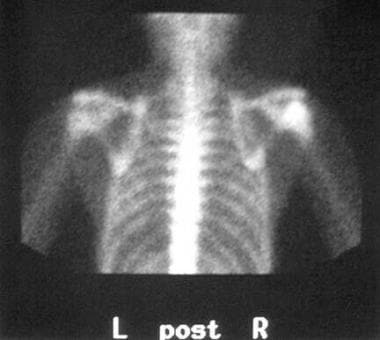 Bone scan of a humeral head chondroblastoma in a 16-year-old girl. Uptake of the bone-seeking agent may be due in part to the regional hyperemia of the tumor.
Bone scan of a humeral head chondroblastoma in a 16-year-old girl. Uptake of the bone-seeking agent may be due in part to the regional hyperemia of the tumor.
In the presence of a periosteal reaction, radionuclide uptake may extend beyond the lesion margins (see the image below). If radionuclide uptake is present in multiple areas, chondroblastomas are less likely than enchondromas or osteochondromas, which are more frequently multiple.
 Bone scan of a proximal humeral chondroblastoma in a 17-year-old boy. In the presence of a periosteal reaction, uptake of the bone-seeking agent may extend beyond the lesion's margins.
Bone scan of a proximal humeral chondroblastoma in a 17-year-old boy. In the presence of a periosteal reaction, uptake of the bone-seeking agent may extend beyond the lesion's margins.
-
Plain radiograph of the distal femoral epiphysis in a 12-year-old boy. This image shows a chondroblastoma with a characteristically lucent lesion and well-defined margins. Extension across the physis was confirmed with computed tomography scanning and magnetic resonance imaging.
-
Coronal reconstructed computed tomography scan of the knee in a 12-year-old boy. This image confirms extension of the chondroblastoma into the metaphysis.
-
Coronal T1-weighted magnetic resonance image of the knee in a 12-year-old boy. This image also confirms extension of the chondroblastoma into the metaphysis.
-
Sagittal T2-weighted magnetic resonance image of the knee in a 12-year-old boy. This image shows extension of the chondroblastoma across the physis. At histologic examination, central foci of low signal intensity, which are common in chondroblastomas, may be correlated with hypercellularity of the chondroblasts, calcification, and/or hemosiderin deposition.
-
Plain radiograph of the proximal tibia in a 14-year-old boy. This image demonstrates a chondroblastoma that has well-circumscribed, thin, sclerotic margins. Chondroblastomas may have sclerotic, nonsclerotic, or incompletely sclerotic borders.
-
Coronal T1-weighted magnetic resonance image of a proximal tibial chondroblastoma in a 14-year-old boy.
-
Coronal T2-weighted magnetic resonance image (MRI) of a proximal tibial chondroblastoma in a 14-year-old boy. The lesion is confined to the epiphysis. The presence of surrounding edema is best depicted with MRI.
-
Plain radiograph of the greater trochanter in a 24-year-old man. Chondroblastomas that occur in the proximal femur are 3 times more likely to occur in the greater trochanter than in the femoral head.
-
Coronal T2-weighted magnetic resonance image of a greater trochanter chondroblastoma in a 24-year-old man.
-
Plain radiograph of the right upper extremity of a 16-year-old girl. This image shows a chondroblastoma in the humeral head.
-
Axial computed tomography scan of a humeral head chondroblastoma in a 16-year-old girl. The mottled central opacity that was demonstrated on the plain radiograph was due to amorphous calcifications within the lesion, which occur in approximately 60% of all chondroblastomas.
-
Bone scan of a humeral head chondroblastoma in a 16-year-old girl. Uptake of the bone-seeking agent may be due in part to the regional hyperemia of the tumor.
-
Plain radiograph of the talus in a 12-year-old boy. About 10% of all chondroblastomas occur in the small bones of the hands and feet. The talus and calcaneus are relatively common sites.
-
Plain radiograph of the pedicle and transverse process of a lumbar vertebra. Although the diagnosis of osteoblastoma was made on the basis of the radiographic appearance of the tumor, chondroblastoma was confirmed at pathologic examination.
-
Axial computed tomography scan of a spinal chondroblastoma. Chondroblastoma rarely occurs in the spine.
-
Axial nonenhanced T1-weighted magnetic resonance image of a spinal chondroblastoma.
-
Contrast-enhanced axial T1-weighted magnetic resonance image of a spinal chondroblastoma. This image shows nonspecific but uniform enhancement throughout the lesion.
-
Oblique plain radiograph of the patella in a 16-year-old girl. Note the presence of a comminuted pathologic fracture in association with the chondroblastoma.
-
Axial computed tomography scan of a patellar chondroblastoma in a 16-year-old girl. This image shows the comminuted pathologic fracture to better advantage.
-
Plain radiograph of the acromion in a 54-year-old man. The chondroblastoma is in an unusual location and is atypically present in an older patient.
-
Plain radiograph of the proximal humerus in a 17-year-old boy. A subtle, solid, adjacent metaphyseal periosteal reaction is present medially due to the chondroblastoma. A metaphyseal periosteal reaction occurs in 15-30% of chondroblastomas.
-
Axial T2-weighted magnetic resonance image of a humeral head chondroblastoma in a 17-year-old boy. Fluid-fluid levels are occasionally seen on images of chondroblastomas, which can simulate aneurysmal bone cysts.
-
Bone scan of a proximal humeral chondroblastoma in a 17-year-old boy. In the presence of a periosteal reaction, uptake of the bone-seeking agent may extend beyond the lesion's margins.


