Practice Essentials
Medial epicondylitis (ME) is an overuse injury affecting the flexor-pronator muscle origin at the anterior medial epicondyle of the humerus. ME is often discussed in conjunction with lateral epicondylitis (LE), which occurs much more frequently. ME is the most common cause of medial elbow pain, although the clinician is likely to see at least 5 cases of LE for every case of ME. Patients who develop medial elbow pain appreciate their physician's knowledge of the subtle differences in the diagnosis and treatment of the two disorders. [1, 2] (See images below.)
 Strengthening exercises are performed once pain has subsided with active range of motion. The starting position (slight pronation) of an eccentric exercise for medial epicondylitis is shown. In order to prevent further injury, a trained therapist should instruct patients in exercises to confirm proper weight and technique.
Strengthening exercises are performed once pain has subsided with active range of motion. The starting position (slight pronation) of an eccentric exercise for medial epicondylitis is shown. In order to prevent further injury, a trained therapist should instruct patients in exercises to confirm proper weight and technique.

Signs and symptoms of medial epicondylitis
ME is characterized by pain over the medial epicondyle. Pain worsens with wrist flexion and forearm pronation activities.
Patients may have symptoms of an ulnar neuropathy (eg, decreased sensation in the ulnar nerve distribution, a positive elbow-flexion test, a positive Tinel sign). In more severe cases, decreased sensation is associated with intrinsic weakness; intrinsic muscle atrophy may be noted.
Workup in medial epicondylitis
Imaging studies
A radiograph of the elbow is often performed to rule out associated lesions (eg, loose bodies, bony avulsion, osteoarthritis). Typically, anteroposterior and lateral films are adequate.
Oblique views are needed if loose bodies are suggested upon examination or because of a catching or clicking sensation described by the patient.
Magnetic resonance imaging (MRI) may be helpful in looking for the characteristic pathology that is seen in chronic cases of ME; MRI also permits assessment of the medial collateral ligament and ulnar nerve. [3]
Other tests
If ulnar nerve involvement is suggested, a nerve conduction study and electromyography should be performed.
Management of medial epicondylitis
Occupational therapy
To decrease pain and inflammation, treatment begins with the following:
-
Rest
-
Ice
-
Compression - Compression with a medial counterforce brace (ie, a tennis elbow splint) with a pad placed anteromedially on the proximal forearm over the flexor-pronator mass is routine
-
Bracing
After the patient's initial discomfort has subsided, a rehabilitation program with an occupational therapist should be initiated for muscle/tendon reconditioning. Begin with gentle stretching and add gradual strengthening of the flexor-pronator muscles, as the patient tolerates. Follow this with functional activities and with patient education aimed at avoiding re-injury.
Concomitant modalities may include the following:
-
Ultrasound
-
Iontophoresis
-
Phonophoresis
-
Transcutaneous electrical nerve stimulation
-
Low-energy, extracorporeal shock-wave therapy
Surgical intervention
Epicondylar debridement is rarely indicated but has proven to be effective in cases in which conservative treatment has failed. In addition, the ulnar nerve may be decompressed surgically. [4]
Injections
If conservative measures fail, injection with local anesthetic and steroid to the point of maximal tenderness is appropriate. Special care should be taken to avoid injection directly into the tendon or the ulnar nerve.
Pathophysiology
ME involves primarily the flexor-pronator muscles (ie, pronator teres, flexor carpi radialis, palmaris longus) at their origin on the anterior medial epicondyle. Less often, ME also affects the flexor carpi ulnaris and flexor digitorum superficialis. Repetitive stress at the musculotendinous junction and its origin at the epicondyle leads to tendinitis in its most acute form and to tendinosis in its more chronic form. [5] In addition, an ulnar neuropraxia caused by compression of the ulnar nerve in or around the medial epicondylar groove has been estimated to occur in up to 50% of ME cases.
The tendinosis that occurs is primarily the result of failure of the damaged tendon to heal. Microscopic examination of the involved tissue shows granulation tissue, fibrovascular and fibrocartilaginous tissue, tendon microfragmentation, calcification, and necrosis. Histologically, damage to the involved tendons has been described as angiofibroblastic hyperplasia tendinosis and fibrillary degeneration of collagen. [6] A simple, acute inflammatory reaction is noted to be a much less common finding than are the previously described tendinosis changes.
Epidemiology
Race
No studies indicate a race predilection.
Sex
A male-to-female ratio of 2:1 has been reported.
Age
Peak incidence is in patients aged 20-49 years, but ME is also seen in teens and older adults, especially if they engage in hobbies, jobs, or sports activities that make them prone to overuse injuries.
-
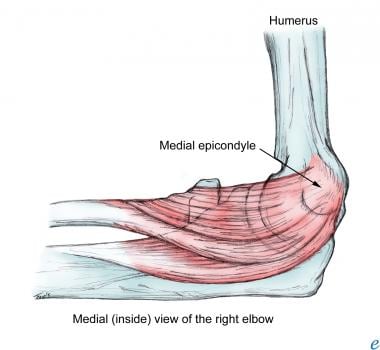
Medial epicondyle.
-
Strengthening exercises are performed once pain has subsided with active range of motion. The starting position (slight pronation) of an eccentric exercise for medial epicondylitis is shown. In order to prevent further injury, a trained therapist should instruct patients in exercises to confirm proper weight and technique.
-
The eccentric exercise proceeds until full supination has been reached.



