Practice Essentials
Thoracic outlet syndrome (TOS) involves compression, injury, or irritation to the neurovascular structures at the root of the neck or upper thoracic region, bounded by the anterior and middle scalenes; between the clavicle and first rib (with possible enlargement/hypertrophy of the subclavius); or beneath the pectoralis minor muscle. Some authors define the thoracic outlet as an opening bordered by the first rib laterally, the vertebral column medially, and the claviculomanubrial complex anteriorly. The syndrome of compression at this site could be primarily neurologic, involving the brachial plexus, most often the lower trunk or medial cord; alternatively, it could involve compression of the subclavian artery and/or vein. [1, 2, 3] Thrombosis, embolus, or aneurysm of these vessels is a less likely possibility. [4, 5]
In addition, imaging with diagnostic ultrasonography has been able to identify deformation of the pectoralis minor in TOS that may be related to the pathophysiology, due to excessive tightness or shortening of the muscle that impinges on the neurovascular bundle. [6]
One proposed classification system broke TOS into the following three categories:
-
True neurogenic TOS - The brachial plexus is injured in these cases as documented by electromyography (EMG) and/or nerve conduction studies
-
Nonspecific or disputed TOS - Patients have symptoms, but there are no abnormal tests to document the lesion clearly. This category is by far the most common type of TOS seen in the clinical setting
In the subsequent literature, however, TOS has been categorized into five clinically distinct variations, based on specific pathophysiology. These include arterial, venous, traumatic neurovascular, true neurogenic, and disputed. In each type, at least one neurovascular element is compressed as it traverses the thoracic outlet. [4, 5]
A new category is recommended for cases in which no objective neurologic or vascular abnormality can be identified. These cases could be termed postural thoracic outlet syndrome, which may be more appropriate, owing to the dysfunctional body habitus observed almost universally in these cases. [7, 8]
TOS is a controversial topic in the literature; many proponents support the existence of the condition, but some strongly vocal opponents doubt the validity of TOS as a medical entity. Even the name itself has been questioned because the actual site of pathology is technically the thoracic "inlet," not the "outlet." The primary controversy seems to center around the lack of objective criteria for diagnosis and the confusion with multiple types or clinical presentations.
Since TOS involves proximal neurovascular structures (see the image below), symptoms often are confused with various distal compression neuropathies or cervical radiculopathies.
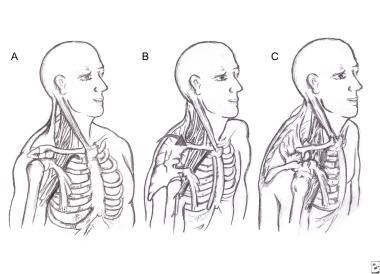 Progressive postural decompensation with neurovascular compression. A: Normal resting posture. B: Shoulder protraction beginning; the sternomastoid muscles are shortening, drawing the head anteriorly and inferiorly. C: Advanced deformity with adaptive shortening of scalene and pectoralis minor muscles. Also note narrowed costoclavicular space (ribs 1-5 have been relatively elevated). Neurovascular compression is evident at all 3 sites.
Progressive postural decompensation with neurovascular compression. A: Normal resting posture. B: Shoulder protraction beginning; the sternomastoid muscles are shortening, drawing the head anteriorly and inferiorly. C: Advanced deformity with adaptive shortening of scalene and pectoralis minor muscles. Also note narrowed costoclavicular space (ribs 1-5 have been relatively elevated). Neurovascular compression is evident at all 3 sites.
In addition, surgical treatment has been known to have devastating complications, which further fuels debate with the opponents of recognition of this entity. Conservative treatment appears to be the most universally accepted approach, with even surgeons recommending a prolonged trial before any operative procedure.
A review of the pathomechanics and dysfunctional body habitus associated with this type of presentation suggests that the term "postural TOS" may be more appropriate, particularly when no neurologic or vascular abnormality is documented (or testing results are inconclusive). [9, 8]
Signs and symptoms of thoracic outlet syndrome
Pain, numbness and/or tingling, and heaviness of the involved upper extremity are common complaints reported by patients with thoracic outlet syndrome (TOS). Often, the symptoms are vague and generalized. The entire extremity may be involved, although a select study of patients with true neurogenic TOS found hypesthesia in the medial forearm or ulnar digits and weakness of the abductor pollicis brevis muscle. [10] Additionally, neck pain and headaches are reported concomitantly. Autonomic phenomena (eg, cold hands, blanching, swelling) also may be reported.
Workup of thoracic outlet syndrome
The most common stress tests in the physical examination diagnosis of thoracic outlet syndrome (TOS) are the Adson maneuvers, where the head is placed in extension and side bending while the patient takes a deep breath and holds it, followed by rotation to stretch or tether the plexus and/or artery by the anterior and middle scalenes.
Radiographs can help to identify cervical ribs, which may be responsible for plexus injury or have associated fibrous bands. Radiographs may also help to identify elevated first ribs, caused by tight, contracted anterior/middle scalene muscles. Displaced clavicle fractures, nonunion, and exuberant callus also can be identified.
A magnetic resonance imaging (MRI) scan of the cervical spine and supraclavicular/brachial plexus area is useful to identify other causes, or a computed tomography (CT) scan of the brachial plexus area and apical lung may be indicated.
MRI and CT scans can identify cervical root injury from degenerative spurs, disc herniation, or other causes.
Other imaging studies that can be used in the assessment of TOS include the following
-
Diagnostic ultrasonographic imaging
-
Doppler and noninvasive blood flow studies
-
Angiography/CT angiography/venography
-
Autonomic assessment (thermography)
EMG and nerve conduction studies, also known as electrodiagnostic studies, are necessary to identify true neurogenic TOS and to rule out other sites of compression neuropathy.
Management
Modalities with deep heat (eg, therapeutic ultrasound), electric stimulation, superficial heat (eg, Hydrocollator packs), stretching exercises, postural correction exercises, and strength and endurance exercises are all useful or necessary components of thoracic outlet syndrome (TOS) treatment.
Mobilization and manipulation procedures (often performed by an osteopathic physician) usually are indicated and necessary to release tight, contracted/restricted vertebral segments and soft tissue (myofascial) regions, especially the anterior/middle scalenes and pectoralis minor muscle entrapment sites.
Generally, surgery is used as a last resort after a prolonged trial (ie, months) of conservative treatment. First rib resection has been advocated by many surgeons to treat TOS. Many also use scalenectomy, in combination with rib removal or as a second procedure, if the initial surgery is ineffective. [11] Resection of accessory ribs and fibrous bands should be performed, especially if observed to be tethering the plexus.
In cases where clavicular fracture is responsible for plexus compression, removal of hyperabundant callus may be necessary.
Pathophysiology
Many authors have discovered accessory cervical ribs associated with TOS [12] ; however, they have noted tough fibrous bands coming off the accessory ribs that are believed to be more responsible for the pathology. There have even been reports of bony fusion of variant cervical ribs, resulting in bifid ribs with attached fibrous bands. [13] The bands cause tethering of the brachial plexus, which results in traction and, therefore, symptoms. Other authors report compression or irritation of the neurovascular bundle more distally under the pectoralis minor muscle or from anterior displacement of the humeral head.
Additionally, clavicle fractures can result in plexopathy from expanding hematomas or pseudoaneurysms that compress the plexus, with variable latent periods following the fracture. Delayed onset of symptoms may suggest exuberant callus from the healing fracture site. Nonunion of the fracture site also can result in direct compression by the lateral fragment, which is pulled inferiorly.
Trapezius weakness due to spinal accessory nerve injury (following cervical lymph node biopsy) also has been implicated as a cause of TOS. This results in "droopy shoulder" with secondary compression of the neurovascular bundle, which is particularly aggravated with arm elevation (abduction). [14]
Epidemiology
Frequency
United States
The inability to make a definitive and accurate diagnosis makes determination of the exact prevalence of this condition impossible. The prevalence of nonspecific thoracic outlet syndrome (TOS) has been reported as high as 23% of soft-tissue injuries of the cervical spine. TOS is overlooked or misdiagnosed commonly, especially upon presentation to the emergency department. The true or classical neurogenic or vascular TOS incidence is considered rare, with only 1 case per million population estimated for the neurogenic type. Some believe that TOS is the most common cause of acute arterial occlusion in the upper limbs of adults younger than 40 years. It is more common with occupations or activities that involve prolonged posturing of the neck, such as secretaries, cashiers, machine operators, surgeons, truck drivers, and overhead work or lifting. There is no increased incidence in athletes.
Mortality/Morbidity
No known mortality is associated directly with thoracic outlet syndrome (TOS). Morbidity often encompasses debilitating functional loss of the involved upper extremity, loss of livelihood or occupation, especially if the work involves overhead activity (eg, hairdressing, carpentry, painting). True neurogenic TOS causes neurologic deficit. Depending on the amount of nerve injury, there usually is weakness of the hand and sensory deficits in the lower trunk distribution. Devastating complications, usually to the brachial plexus, have been reported from surgical treatment for TOS.
Sex
Females are diagnosed more commonly with thoracic outlet syndrome than males, with some reports of a 9:1 female-to-male ratio. The shape of the chest wall is believed to predispose women by encouraging closure of the thoracic outlet. Large, pendulous breasts have been particularly implicated, with these adding to the anterior forces on the chest, leading to drooped shoulder posturing and further closing the outlet. [14]
Age
Age of onset of thoracic outlet syndrome is from the second to the eighth decade, with a peak occurring in the fourth decade. In the younger age group, there appears to be a greater likelihood of anatomic or structural abnormality, such as cervical rib variants and fibrous bands.
-
Progressive postural decompensation with neurovascular compression. A: Normal resting posture. B: Shoulder protraction beginning; the sternomastoid muscles are shortening, drawing the head anteriorly and inferiorly. C: Advanced deformity with adaptive shortening of scalene and pectoralis minor muscles. Also note narrowed costoclavicular space (ribs 1-5 have been relatively elevated). Neurovascular compression is evident at all 3 sites.
-
Scalene focal (left) and regional (right) stress tests for thoracic outlet syndrome. Both tests can be easily combined to enhance the stress effect (may be helpful in mild cases).
-
Pectoral focal (left) and regional (right) stress tests for thoracic outlet syndrome.
-
Stretching technique for the pectoralis minor muscle. Left: The patient has taken the slack out of the muscle. Center: He then rotates the body away from the side being stretched, increasing traction. Right: Maximum rotation and stretch effect are achieved slowly. Image courtesy of The Journal of the American Osteopathic Association
-
Sagittal plane posture of patient with thoracic outlet syndrome before (left) and after (right) treatment. Notice the release of the pelvis that occurred with the reduction in hyperlordosis, which allowed the shoulder girdle to drop back and open the thoracic outlet. Image courtesy of The Journal of the American Osteopathic Association
-
Myofascial release technique for the scalene muscles. Left: Side-lying approach. Right/top: Supine approach with pillow under thorax. Right/bottom: Supine approach with head extended off the table and supported by the operator's knees. Image courtesy of The Journal of the American Osteopathic Association
-
Stretching technique for the scalene (anterior and middle) muscles. Left: The arm on the side to be stretched is secured down (hooked under the seat) to allow more control and effective stretch. Center: The opposite hand wraps partially around the head for good control to assist with the stretch. Right: After proceeding as far as tolerated, the patient leans the whole trunk away from the side being stretched, creating additional traction (downward) on the muscle by the arm that is secured. Image courtesy of The Journal of the American Osteopathic Association
-
Algorithm for the treatment of nonprogressive thoracic outlet syndrome (TOS). Anti-inflammatory medication, muscle relaxants, and activity modifications all are used as indicated and tolerated in all cases. Values for very severe TOS are greater than those for severe TOS, and the patient probably should be referred for surgical evaluation.






