Practice Essentials
Helicobacter pylori is a gram-negative bacillus responsible for one of the most common infections found in humans worldwide. [1] (See the image below.) Children differ from adults with respect to H pylori infection in terms of the prevalence of the infection, the complication rate, the near-absence of gastric malignancies, age-specific problems with diagnostic tests and drugs, and a higher rate of antibiotic resistance. These and other differences explain why some of the recommendations for adults may not apply in children. [2]

Signs and symptoms
Most children infected with H pylori are asymptomatic. Antral gastritis is the most common manifestation in children. A history of anorexia and weight loss, pallor or laboratory findings of anemia, vomiting, abdominal pain associated with meals or nighttime, and any description of GI bleeding raises concern for peptic ulcer disease.
See Presentation for more detail.
Diagnosis
Testing for H pylori should be performed in children with gastric or duodenal ulcers.
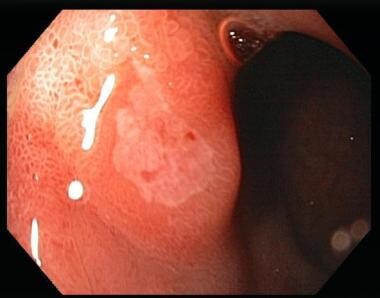
Upper endoscopy is the procedure of choice for detecting gastritis, duodenitis, and peptic ulcer disease in children and adolescents.
See Workup for more detail.
Management
For first-line therapy for H pylori infection, if the strain is susceptible to clarithromycin (CLA) and to metronidazole (MET), triple therapy (proton pump inhibitor [PPI], amoxicillin [AMO], CLA) for 14 days is the preferred choice. Sequential therapy for 10 days (PPI with AMO for 5 days, followed by PPI with CLA and MET for 5 days) is equally effective in patients infected with fully susceptible strains. However, sequential therapy has the disadvantage of exposing the child to three different antibiotics. [3]
Antibiotic resistance is the major cause of failure in the treatment of H pylori infection. As a result, recommended therapies should be based on antibiotic susceptibility testing.
When antibiotic susceptibility profiles are not known, high-dose triple therapy with PPI, AMO, and MET for 14 days is recommended as first-line therapy. Bismuth-based quadruple therapy can also be considered for first-line therapy in countries where it is licensed for use in children.
See Treatment and Medication for more detail.
Background
Warren and Marshall first cultured and identified Helicobacter pylori as Campylobacter pylori in 1982. By 1989, it was renamed and recognized to be associated closely with antral gastritis (gastric and duodenal ulcers in adults and children). In recognition of this crucial discovery, they were awarded the Nobel Prize for medicine in 2005. By the early-to-mid 1990s, further evidence supported a link between chronic gastritis of H pylori infection in adults and malignancy, specifically gastric lymphoma and adenocarcinoma.
A fascinating study using the ability of molecular fingerprinting (multilocus sequence typing [MLST]) reported on following the spread of H pylori by human ancestral roots from Africa. Moodley et al estimated that H pylori is approximately as old as modern humans and that migration out of Africa occurred in several waves, the first one 60,000 years ago and the second 52,000 years ago. [4]
Objectives of current and future research on H pylori include improving the understanding of the immunopathogenesis of gastric disease associated with H pylori infection, elucidating the modes of transmission, and improving the safety and efficacy of vaccines to prevent H pylori infection. (See the image below.)
Pathophysiology
H pylori organisms are spiral-shaped gram-negative bacteria that are highly motile because of multiple unipolar flagella. They are microaerophilic and potent producers of the enzyme urease. H pylori inhabits the mucus adjacent to the gastric mucosa.
Important adaptive features that enhance survival of the organism in an acidic environment include its shape and motility, its reduced oxygen requirement, its adhesion molecules that are trophic to certain gastric cells, and its urease production. Bacterial urease converts urea to ammonium and bicarbonate, neutralizing gastric acid and providing protection in the hostile, highly acidic gastric environment. Some of the lipopolysaccharide of the organism mimics the Lewis blood group antigens in structure. This molecular mimicry also helps in the continued existence of H pylori in the unfavorable gastric environment. [5]
H pylori produces suspected disease-inducing factors, including urease, vacuolating cytotoxin, catalase, and lipopolysaccharide (LPS). Urease, a potent antigen, induces increased immunoglobulin G and immunoglobulin A production. Expression of vacuolating cytotoxin, which induces inflammatory cytokines, may be associated with more pronounced inflammation and increased propensity to cause disease. Catalase helps H pylori survive in the host by preventing the formation of reactive oxygen metabolites from hydrogen peroxide. The LPS outer membrane of H pylori is a less potent inducer of the host complement cascade.
Cytotoxin-associated antigen (CagA) is probably the most important virulence factor in H pylori infection . An individual infected with CagA-negative strains is likely only to develop chronic gastritis and have only a small chance of developing peptic ulcer disease or gastric cancer. In contrast, infection with CagA-positive strains greatly increases the risk of peptic ulcer disease and gastric cancer. Translocating the CagA protein into the gastric epithelial cells causes rearrangement of the host cytoskeleton and alters cell signaling and perturbs cell cycle control. Furthermore, CagA-positive strains are known to induce the expression of a DNA-editing enzyme, which leads to accumulation of mutations in the tumor suppressor p53. [6]
CagA in situ expression is increased in children with H pylori infection who have peptic ulcers and may play a role in the pathogenesis of peptic ulcer disease (PUD). [7]
CagA can be divided in 2 types, the East-Asian type and the Western type, according to the repeat sequences of the 3′ region of cagA. Individuals infected with East-Asian type cagA strains are reported to have higher risk of PUD or gastric cancer than those with Western-type cagA strains. [8]
The association between serum anti-CagA antibodies and gastric cancer in East Asian countries (Japan, Korea, and China) was clarified in a meta-analysis of case-control studies with age and sex-matched controls, in which 10 studies with a total of 4325 patients were identified. [9] CagA seropositivity was associated with gastric cancer compared with gastritis, even in East Asian countries, although the odds ratio (OR) in East Asian countries was smaller than that of another meta-analysis, which included Western countries.
Duodenal ulcer–promoting gene (DupA) is the first genetic factor of H pylori detected to be associated with a differential susceptibility to duodenal ulcer and gastric cancer. Thus, it can be considered a disease-specific virulence marker. [8] The prevalence of dupA was significantly higher in strains from patients with duodenal ulcer but lower in those with gastric cancer (42% vs 9%, on average).
H pylori colonizes the stomach, induces inflammatory cytokines, and causes gastric inflammation. Individuals with H pylori– associated antral-predominant gastritis with increased gastric acid production are prone to PUD. [10] In contrast, H pylori pan-predominant gastritis or corpus-predominant gastritis with decreased gastric acid production are more prone to developing gastric atrophy (intestinal metaplasia and gastric adenocarcinoma).
H pylori has been associated with iron-deficiency anemia. The 2 main hypotheses that potentially explain this relation are (1) sequestration of iron due to antral H pylori infection and (2) decreased non-heme iron absorption caused by hypochlorhydria.
H pylori infection and its association with gastric malignancy have been well described in several epidemiologic studies. [11] However, the course of progression from inflammation to cancer remains unclear. One model describes the stepwise progression of H pylori infection to hypochlorhydria, chronic gastritis, atrophic gastritis, intestinal metaplasia, and gastric cancer. Increased production of the cytokine interleukin 1β has been linked to an increased risk of hypochlorhydria and gastric cancer in infected subjects.
A study found that helicobacter pylori increases cellular proliferation and alters tight junctions by changing the expression of several cancer-related proteins such as beta-catenin, claudin-7, and snail. [12]
A growing area of research interest investigates the hypothesis that H pylori infection may be protective against autoinflammatory diseases such as asthma or inflammatory bowel disease. For example, epidemiologic data suggest that H pylori infection is less common in patients with inflammatory bowel disease, leading investigators to delineate the potential mechanisms underlying these clinical findings.
Etiology
Epidemiologic studies have addressed various factors, such as bacterial, host, genetic, and environmental factors, to determine the causative links to H pylori infection. Data support person-to-person spread of infection, possibly related to dental plaque, but knowledge of reservoirs and transmission modes is incomplete.
Causes of H pylori infection include the following:
-
Person-to-person transmission of H pylori infection is noted.
Infection clusters are noted, particularly in families with infected children. The possible routes are fecal-oral, oral-oral and gastro-oral. Mother-to-child transmission was strongly suggested in a study of DNA analysis of the H pylori strains. [13] The data showed identical H pylori strains between mothers and their toddler-aged children. Moreover, the mother’s symptoms of nausea and vomiting and the use of pacifier were significantly associated with the risk of H pylori infection in children.
In a very interesting longitudinal study from the US-Mexican border, Cervantes et al showed that a younger sibling was 4 times more likely to become infected with H pylori if the mother was infected with H pylori compared with an uninfected mother. Younger siblings were 8 times more likely to become infected if their older index sibling had persistent H pylori infection. [14]
The possibility of H pylori transmission among children in daycare centers or kindergarten, where interpersonal contacts are common, was also proposed. A meta-analysis of 16 studies did not confirm this hypothesis. The summary OR was 1.12 (95% confidence interval, 0.82–1.52). However, the authors highlighted the limitations of the published studies, including different types of childcare, different age groups, and lack of differences in the exposure duration, with exposure giving a high heterogeneity to the meta-analysis results. [15]
Crowding and poor personal hygiene may also play a role.
An increased prevalence of H pylori infection is noted in developing countries. This may reflect the combined effects of poor living conditions, poor hygiene, and crowding.
In the United States, socioeconomic level is strongly and inversely related to the prevalence of H pylori infection, a finding that may also reflect the same factors as those noted in developing countries.
-
Bacterial factors may play a role in the clinical manifestations of H pylori infection.
Patients with H pylori infection have 2 basic phenotypes based on the presence or absence of a vacuolating cytotoxin.
People with cytotoxin-positive infection have endoscopically proven inflammation that is more pronounced than those of patients with cytotoxin-negative H pylori infection.
-
Host factors may play a role in the acquisition of H pylori infection.
Children may be better able to clear acute infection than adults (2% per year).
Hypochlorhydria may be necessary to allow H pylori to colonize in the stomach.
Normal gastric epithelial cells that line the stomach are necessary for H pylori persistence. H pylori is not found in atrophied metaplastic epithelium.
-
Data from only one study links an increased prevalence of H pylori infection with a community's water supply. [16]
-
Other possible ways of transmission include vector-borne transmission. [17]
-
H pylori isolates are found more often in personnel who work in the endoscopy suite than in the general population.
Epidemiology
United States statistics
Overall, approximately one-third of the population is infected with H pylori, increasing with age.
International statistics
In general, the prevalence is high in developing countries and the infection is acquired at a young age. The incidence is 3-10% of the population each year in developing countries compared with 0.5% in developed countries. [18] The prevalence of H pylori infection is not only lower in industrialized countries than in developing countries, but the incidence of H pylori infection, gastric cancer, and ulcer disease are also declining. Worldwide, more than 1 billion people are estimated to be infected with H pylori.
A systematic review and meta-analysis by Yuan et al found that the overall prevalence of H pylori infection in children worldwide is 32.3%. The researchers also demonstrated that the prevalence of H pylori infection in children in low-income and middle-income countries (43.2%) is nearly twice the prevalence in high-income countries (21.7%). [19]
Race-, sex-, and age-related demographics
The prevalence is increased in Black, Hispanic, Asian, and Native American populations.
Infection rates are similar in males and females.
In developed countries, less than 10% of children younger than 12 years are infected; however, seropositivity increases with age at a rate of 0.3-1% per year. Studies of seropositivity in adults in developed countries revealed prevalences of 30-50%. In the United States, the estimated prevalence is 20% for people younger than 30 years and 50% for those older than 60 years. In developing countries, the prevalence rates are much higher. The serological prevalence rates of H pylori were 15% and 46% in Gambian children younger than 20 months and age 40-60 months, respectively. [20]
Muhsen et al examined the age of acquisition of H pylori infection in a prospective study on Israeli Arab children in 2 villages with different socioeconomic statuses. Prevalence was 6% in the high socioeconomic status village and 10% in the low socioeconomic village in the first 6 months of life; at 18 months, it increased to 9.6% and 51.9%, respectively. [21]
Prognosis
The outlook for eradicating H pylori infection with multidrug therapy is good, with reported efficacy rates as high as 95%.
Unsuccessful therapy often results from the patient's noncompliance with the medication regimen or from antimicrobial resistance.
Once cure is achieved, long-term reinfection rates are low. Among children living in developing countries or among families with infected members, reinfection rates may be increased.
Morbidity/mortality
Most children infected with H pylori are asymptomatic. Antral gastritis is the most common manifestation in children. Duodenal and gastric ulcers may be associated with H pylori gastritis in adults but is uncommon in children. The risk of gastric cancers, including non-Hodgkin lymphoma (eg, mucosa-associated lymphoid tissue [MALT]) and adenocarcinoma, is increased in adults. A study by Lee et al associated eradication of H pylori infection with a reduced incidence of gastric cancer. [22, 23]
The majority of studies have reported a decrease in the incidence and/or prevalence of PUD over time, presumably because of a decrease in H pylori –associated PUD. H pylori was initially responsible for up to 95% of all gastroduodenal ulcers, but more recent studies have reported that the prevalence of H pylori in patients with PUD ranges from 36-73%, depending on ethnicity, geographic factors, and socioeconomic factors. [24]
The relationship between H pylori gastritis and recurrent abdominal pain (RAP) is controversial. The incidence of H pylori gastritis in patients with RAP is not significantly higher than the incidence of H pylori infection in the general population. Although some studies demonstrate an improvement in symptoms in children with RAP and H pylori gastritis after eradication therapy for H pylori, data from a recent double-blind controlled trial did not confirm that finding. [25] The heterogenicity of their definition of RAP and the varying study methodologies may have led to different results and conclusions. The medical positional statement of the North American Society of Pediatric Gastroenterology, Hepatology, and Nutrition regarding H pylori infection in children also found no convincing data to support the routine testing of children with RAP for H pylori. [26]
A meta-analysis reviewed published evidence for an association between H pylori infection and GI symptoms in children and found no association between RAP and H pylori infection and found conflicting evidence for an association between epigastric pain and H pylori infection. [27]
Some studies suggest that H pylori protects human subjects from developing gastroesophageal reflux disease, whereas others postulate a causative association between them. A meta-analysis of studies in adults found no association between H pylori eradication and development of new cases of gastroesophageal reflux disease in the population of dyspeptic patients. [28]
One pediatric retrospective study revealed a significantly higher prevalence of reflux esophagitis in children with H pylori infection. [29]
A meta-analysis summarized the existing literature examining the effect that H pylori has on Barrett esophagus. Only few studies without obvious selection and information bias have been conducted to examine the effect of H pylori on Barrett esophagus, but, in these, H pylori infection is associated with a reduced risk of Barrett esophagus. [30]
Controversy exists concerning the relationship of H pylori infection and somatic growth retardation in children. The gastrointestinal hormone ghrelin is a gut-brain peptide that regulates food intake in humans and has strong growth hormone–releasing activity. Decreased appetite in H pylori –infected children has been related to low plasma ghrelin levels, which returned to normal after H pylori eradication. [31]
H pylori infection has also been associated with extraintestinal manifestations, such as immune thrombocytopenic purpura. For adults with immune thrombocytopenic purpura, systematic reviews of past literature have shown an overall platelet response in more than 50% of the patients successfully treated for the infection and increased response rates in countries with a high prevalence of H pylori infection in background populations. [32]
Complications
Complications of H pylori infection include the following:
-
PUD - Perforation, GI bleeding
-
Iron-deficiency anemia
-
Malignancy
Gastric mucosa-associated lymphoid tissue (MALT) lymphoma
Adenocarcinoma of the gastric body and antrum
-
Gastric-outlet obstruction
-
Increased susceptibility to enteric infections such as salmonellosis and giardiasis due to H pylori- induced hypochlorhydria
Patient Education
At present, the nature of transmission of H pylori infection is not fully understood. Therefore, the ability to implement appropriate infection control or preventive measures is limited.
The theory that H pylori requires person-to-person transmission, supported by data from epidemiologic studies, may prove instrumental in promoting policies that improve living conditions and sanitation and to reduce crowding.
The true effect of educational efforts to reduce H pylori transmission in the patient's family (eg, teaching children about appropriate hygiene and toilet practices) is unknown. However, such efforts may be a part of a common-sense approach to reducing transmission of all pathogens infecting the GI tract.
-
Helicobacter pylori infection revealed by endoscopy (nodular gastropathy).
-
Helicobacter pylori–associated peptic ulcer in the duodenal bulb.








