Practice Essentials
First described by Peters et al in 1950, cerebral salt-wasting syndrome is defined by the development of extracellular volume depletion due to a renal sodium transport abnormality in patients with intracranial disease and normal adrenal and thyroid function. [1, 2] As such, it may be more appropriately termed renal salt wasting. Complications of cerebral salt-wasting syndrome include symptomatic hyponatremia and dehydration. (See Pathophysiology, Etiology, and Presentation.) Management of cerebral salt-wasting syndrome centers on correction of intravascular volume depletion and hyponatremia, as well as on replacement of ongoing urinary sodium loss, usually with intravenous (IV) hypertonic saline solutions. [3]
Differentiation of this disorder from the syndrome of inappropriate antidiuretic hormone secretion (SIADH), a common cause of hyponatremia, can be difficult because both can present with hyponatremia and concentrated urine with natriuresis. However, distinguishing between the two disorders is important because treatment options differ. Attention to the volume status of the patient is important in making the distinction. Failure to distinguish cerebral salt-wasting syndrome from SIADH in a patient with hyponatremia who has brain injury could lead to inappropriate therapy with fluid restriction. (See Presentation and Workup.)
Although the diagnosis of cerebral salt-wasting syndrome is thought to be controversial by some, [4] it should be considered a discrete clinical entity and may be more common than perceived. [5] It should also be considered in patients without cerebral disease. [4, 6] Possible mechanisms for cerebral salt-wasting syndrome are shown in the chart below.
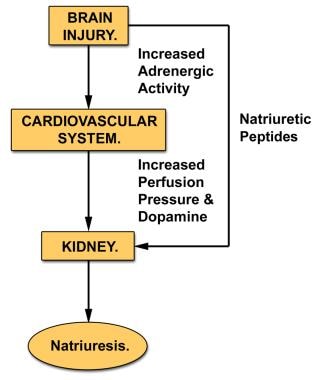 Possible mechanisms for cerebral salt-wasting syndrome. The injured brain may release natriuretic proteins that act directly on the kidney. In addition, cerebral injury may increase sympathetic nervous system activity, elevating renal perfusion pressure and releasing dopamine.
Possible mechanisms for cerebral salt-wasting syndrome. The injured brain may release natriuretic proteins that act directly on the kidney. In addition, cerebral injury may increase sympathetic nervous system activity, elevating renal perfusion pressure and releasing dopamine.
Signs and symptoms of cerebral salt-wasting syndrome
Physical signs of cerebral salt-wasting syndrome (renal salt wasting) include those associated with severe hyponatremia or intravascular volume depletion.
Hyponatremia can be indicated by acute central nervous system (CNS) dysfunction, such as altered mental status, seizures, and coma.
The differentiation of SIADH from cerebral salt-wasting syndrome depends on an accurate estimation of extracellular volume. Unfortunately, no single physical finding can accurately and reproducibly measure effective circulating volume. Commonly used signs of hypovolemia include the following:
-
Orthostatic tachycardia or hypotension
-
Increased capillary refill time
-
Increased skin turgor
-
Dry mucous membranes
-
A sunken anterior fontanelle
These signs usually appear only when the degree of dehydration is moderate to severe. Central venous pressure may be an unreliable determinant of extracellular volume.
Workup in cerebral salt-wasting syndrome
The following lab studies may be indicated in patients with cerebral salt-wasting syndrome:
-
Serum sodium concentration - Patients with untreated cerebral salt-wasting syndrome are often hyponatremic
-
Serum osmolality - If measured serum osmolality exceeds twice the serum sodium concentration and azotemia is not present, suspect hyperglycemia or mannitol as the cause of hyponatremia
-
Urinary output - Urine flow rate is often high in cerebral salt-wasting syndrome; urine flow rate is low in SIADH
Management
Evaluation and treatment of cerebral salt-wasting syndrome, or renal salt wasting, typically occurs in the inpatient setting because most patients are seriously ill with acute CNS disease.
Management centers on correction of intravascular volume depletion and hyponatremia, as well as on replacement of ongoing urinary sodium loss, usually with intravenous (IV) hypertonic saline solutions. [3] Some clinicians have reported a favorable response to mineralocorticoid therapy in cerebral salt-wasting syndrome. Once the patient is stabilized, enteral salt supplementation can be considered.
Pathophysiology
Cerebral salt-wasting syndrome, or renal salt wasting, may be more common than SIADH and may even occur in the absence of cerebral disease. [4, 5, 7] Although the exact mechanism that underlies the development of cerebral salt-wasting syndrome is unclear, it is known that the initiating defect in renal sodium transport leads to extracellular volume depletion and that a cascade of compensatory changes occurs.
Abnormalities in the proximal tubule result in excessive sodium losses, which lead to decreased effective circulating volume. This activates baroreceptors, which increase antidiuretic hormone (ADH) secretion. This results in water conservation and a return to an equilibrated state. In contrast, SIADH primarily occurs due to an inappropriate euvolemic rise in ADH secretion.
The relationship among serum urate, fractional excretion of urate, and hyponatremia in cerebral salt-wasting syndrome is unclear. Fractional excretion of urate may remain elevated even after correction of hyponatremia in patients with cerebral salt-wasting syndrome. This is distinct from SIADH, in which the fractional excretion of urate returns to the reference range once the hyponatremia is corrected. [6] The physiologic basis for this in cerebral salt-wasting syndrome may be related to the receptor-mediated processing of sodium and urate in the proximal tubule, which may be defective in this syndrome. The physiologic basis for hypouricemia in SIADH remains unclear.
The abnormalities in proximal tubular transport may be secondary to a plasma natriuretic factor that reduces proximal and, possibly, distal sodium transport in cerebral salt-wasting syndrome. It may also inhibit the tubular transport of urate, phosphate, and urea in addition to sodium. [8]
Etiology
Cerebral salt-wasting syndrome, or renal salt wasting, occurs in the setting of acute central nervous system (CNS) disease. Conditions leading to cerebral salt-wasting syndrome include the following:
-
Head injury
-
Brain tumor
-
Intracranial surgery
-
Stroke
-
Intracerebral hemorrhage [9]
-
Tuberculous meningitis
-
Craniosynostosis repair
Cerebral salt-wasting syndrome can also occur in the absence of cerebral disease. [7]
The exact mechanism underlying cerebral salt-wasting syndrome remains unclear. In the setting of cerebral injury, one hypothesis is that an exaggerated renal pressure–natriuresis response caused by increased activity of the sympathetic nervous system and dopamine release is responsible for urinary sodium loss.
Another hypothesis involves the release of natriuretic factors, possibly including brain natriuretic peptide (C-type natriuretic peptide) or urodilatin by the injured brain. Kojima et al have described an animal model of cerebral salt-wasting syndrome that may allow better clarification of the condition’s etiology. [10]
A study by Léveillé et al indicated that in persons with traumatic brain injury, risk factors for subsequent significant hyponatremia include a diffuse injury pattern on computed tomography (CT) scan, the presence of multiple lesions on CT scan, and intracerebral hemorrhage. [11]
Epidemiology
Occurrence in the United States
Exact incidence data for this disorder are not available. Approximately 60% of children with brain injuries or tumors develop hyponatremia during their hospital course. Some experts suggest that cerebral salt-wasting syndrome (renal salt wasting) is responsible for hyponatremia at least as often as SIADH is, particularly in neurosurgical patients. Other studies indicate that this syndrome explains the development of hyponatremia in no more than 6% of patients with acute brain injuries. [12] A literature review by Leonard et al found the incidence of cerebral salt-wasting syndrome reported in traumatic brain injury to vary between 0.8-34.6%, with the studies determining these incidences differing with respect to the populations evaluated and the definitions used for hyponatremia and cerebral salt wasting. [13] The exact incidence of renal salt-wasting syndrome without cerebral disease is also unknown.
Age-related demographics
Cerebral salt-wasting syndrome can occur at any age. Published reports include patients aged 6 months to 65 years.
Mortality/morbidity
A study by Kalita et al suggested that cerebral salt wasting is the most frequent cause of stroke-related hyponatremia. The study, of 100 patients with stroke, including 47% with ischemic stroke and 53% with intracerebral hemorrhage, found that 43% of the stroke patients had hyponatremia. Of these, 19 (44.2%) had cerebral salt wasting, while 3 (7.0%) had SIADH, 14 (32.6%) had miscellaneous causes of hyponatremia, and 7 (16.3%) had indeterminate causes of the condition. The investigators also found that length of hospital stay independently predicted the development of cerebral salt wasting and hyponatremia. [14]
A study by Misra et al suggested that in patients with tuberculous meningitis, hypovolemia associated with cerebral salt wasting may play a role in the occurrence of stroke. The report included 81 individuals with tuberculous meningitis, 39.5% of whom suffered ischemic stroke; 50% of these stroke patients had cerebral salt wasting. [15]
Prognosis
Cerebral salt-wasting syndrome usually develops in the first week following a brain insult. Its duration is usually brief (spontaneously resolves in 2-4 wk), although it can last for several months. Death and complication rates for this syndrome are not available. (See Treatment and Medication.)
-
Possible mechanisms for cerebral salt-wasting syndrome. The injured brain may release natriuretic proteins that act directly on the kidney. In addition, cerebral injury may increase sympathetic nervous system activity, elevating renal perfusion pressure and releasing dopamine.

