Practice Essentials
Clear cell sarcoma of the kidney (CCSK) is an uncommon renal neoplasm of childhood. It typically presents as a large unicentric mass markedly distorting or almost completely replacing the kidney (see the image below). Radical nephrectomy is the initial treatment of choice if the lesion is resectable.
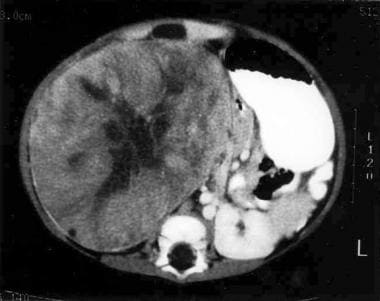 Large right-sided heterogeneous renal mass in a 9-month-old infant. Biopsy findings were consistent with clear cell sarcoma of the kidney.
Large right-sided heterogeneous renal mass in a 9-month-old infant. Biopsy findings were consistent with clear cell sarcoma of the kidney.
Signs and symptoms
Common clinical features include the following:
-
Large palpable unilateral abdominal mass
-
Abdominal pain
-
Hematuria
-
Fever
-
Hypertension
See Presentation for more detail.
Diagnosis
Laboratory studies
Although no specific laboratory result confirms the diagnosis of CCSK, the following investigations should be included in the workup:
-
Complete blood cell (CBC) count
-
Serum creatinine levels
-
Standard preoperative laboratory studies
Imaging studies
No radiologic features can reliably distinguish CCSK from other pediatric renal tumors. However, to define the extent of the tumor, computed tomography (CT) scans of the chest (before surgery) and abdomen should be performed initially.
Histologic findings
Histologically, CCSK shows the following three components:
-
Cord cells
-
Septal cells
-
An intercellular matrix composed of mucopolysaccharide
See Workup for more detail.
Management
At presentation, the treatment of choice is radical nephrectomy if the tumor is resectable. If its size or extension is uncertain, biopsy is performed and chemotherapy administered, followed by surgical resection after a response has been obtained.
See Treatment and Medication for more detail.
Background
Clear cell sarcoma of the kidney (CCSK) represents one of the most common tumors with "unfavorable histology" listed in the National Wilms Tumor Study Group (NWTSG) clinical protocols. [1] In 1970, Kidd initially recognized clear cell sarcoma of the kidney as a distinct clinicopathologic entity, noting its propensity to metastasize to bone. The distinctive histopathologic features of clear cell sarcoma of the kidney were reported simultaneously in 1978 by Morgan and Kidd, [2] Marsden et al, [3] and Beckwith and Palmer. [1] These reports confirmed the propensity of the tumor to metastasize to bone, poor clinical outcome, and the sarcomatous nonepithelial nature of the tumor.
Pathophysiology
Unlike Wilms tumor, clear cell sarcoma of the kidney has not been associated with intralobar nephrogenic rests. In a series of 351 cases from the NWTSG that was reviewed by Argani et al, only one case of clear cell sarcoma of the kidney was associated with a perilobar nephrogenic rest. [4] Gene expression profiles of clear cell sarcomas of the kidney suggest the cell of origin to be a renal mesenchymal cell with neural markers. Only one case has been associated with renal dysplasia, and no familial cases or syndromes have been identified in association with clear cell sarcoma of the kidney. Using the fifth National Wilms Tumor Study (NWTS-5) criteria for tumor staging, 25% of patients had localized stage I tumors, most patients presented with stage II (37%) or stage III (34%) disease, and only 4% of patients presented with distant metastases (see Wilms Tumor for staging information). [5]
Patients presenting with bilateral CCSK at diagnosis are rare but have been reported. [6, 7]
The most common site of metastasis at the time of presentation in patients with clear cell sarcoma of the kidney is the ipsilateral renal hilar lymph nodes. Skip metastases to periaortic lymph nodes have been reported in patients with clear cell sarcoma of the kidney in the presence of hilar lymph nodes that were histologically confirmed with negative results.
Approximately 5% of patients present with distant metastases. Bone is the most common distant site of metastases (15%), followed closely by lung, abdomen, retroperitoneum, brain, and liver. Unusual soft tissue sites (scalp, epidural, nasopharynx, neck, paraspinal, ovary, abdominal wall, axilla) and other sites (orbit) have been reported. Approximately 20% of documented clear cell sarcoma of the kidney metastases occurred at least 3 years after diagnosis; some occurred as long as 10 years later. [8, 9]
Etiology
The histogenesis of clear cell sarcoma of the kidney is unclear and appears to be unrelated to Wilms tumor.
Genomics of clear cell sarcoma of the kidney
Several biological features of clear cell sarcoma of the kidney have been described. They include the following:
-
Internal tandem duplications in exon 15 of the BCOR gene (BCL6 corepressor) were reported in 100% (20 of 20 cases) of clear cell sarcoma of the kidney cases but in none of the other pediatric renal tumors evaluated. [10] Other reports have confirmed the finding of BCOR internal tandem duplications in clear cell sarcoma of the kidney. [11, 12, 13] Hence, BCOR internal tandem duplications appear to play a key role in the tumorigenesis of clear cell sarcoma of the kidney, and their identification should aid in the differential diagnosis of renal tumors. [10]
-
The YWHAE-NUTM2 fusion (involving either NUTM2B or NUTM2E) resulting from t(10;17) was reported in 12% of cases of clear cell sarcoma of the kidney. [14] The presence of the YWHAE-NUTM2 fusion appears to be mutually exclusive with the presence of BCOR internal tandem duplications; this observation is based on a study of 22 cases of clear cell sarcoma of the kidney that included two cases with the YWHAE-NUTM2 fusion and 20 cases with BCOR internal tandem duplications. [11] The gene expression profiles for cases with the YWHAE-NUTM2 fusion were distinctive from those with BCOR internal tandem duplications.
-
The t(10;17)q22;p13) results in an in-frame fusion of the genes YWHA (encoding14-3-3ɛ) and NUTM2 as fusion partners in the resultant in-frame transcript. [14] This fusion protein confers migratory advantage on cells through the up-regulation of EGFR, IGF1R or PDGFα. By blocking these pathways using neutralizing antibodies, the migratory advantage conferred by the transcript was abrogated. This holds potential for novel therapeutic approaches in CCSK. [15]
-
Evaluation of 13 clear cell sarcoma of the kidney tumors for changes in chromosome copy number, mutations, and rearrangements found a single case with the YWHAE-NUTM2 fusion and 12 cases with BCOR internal tandem duplications. [13, 16] No other recurrent segmental chromosomal copy number changes or somatic variants (single nucleotide or small insertion/deletion) were identified, providing further support for the role of BCOR internal tandem duplication as the primary oncogenic driver for clear cell sarcoma of the kidney. [16]
Epidemiology
United States statistics
Clear cell sarcoma of the kidney represents less than 3% of pediatric renal tumors. Approximately 20 new cases are diagnosed each year in the United States. Clear cell sarcoma of the kidney is extremely rare in infants younger than 6 months and in young adults. Most patients are aged 1-4 years. A male predominance is observed. Fifty percent of cases are diagnosed in children aged 2-3 years. Around 5% of patients have metastatic disease at presentation.
International statistics
Hadley et al concluded that in a developing country, such as South Africa, the disease is rare, clinically and radiologically indistinguishable from Wilms tumor, and commonly accompanied by hypertension. Treatment results are poor and difficult to sustain. [17]
Race-, sex-, and age-related demographics
Whites and Blacks are affected in equal numbers.
A male predominance has been noted, with a male-to-female ratio of 2.04:1.
Age of presentation ranges from 2 months to 14 years, with a mean age of 36 months. The highest incidence of clear cell sarcoma of the kidney is in children aged 2-3 years, in which 50% of the cases are diagnosed. A sharp decline in incidence occurs in children older than 3 years. Clear cell sarcoma of the kidney is extremely rare in infants younger than 6 months and in young adults, although it has been reported. The oldest reported patient was aged 57 years. [18] Zhang et al reported the case of a 62-year-old man with clear cell sarcoma of the kidney, who presented with generalized pruritus. [19]
Prognosis
Patients who have stage I tumors, are aged 2-4 years, and have no tumor necrosis tend to have a better prognosis. [20]
Patients who present with distant metastases or multifocal disease have a poor prognosis, with a 50% long-term 6-year survival rate.
An Austrian study found that the most common site of relapse associated with poor survival was the brain. [21]
Treatment with doxorubicin has resulted in a 66% reduction in the tumor-related mortality rate.
Morbidity/mortality
In the fourth National Wilms Tumor Study (NWTS-4), patients were randomized between 6 months of chemotherapy and 15 months of chemotherapy. [22] Patients randomized to 15 months of therapy had a better outcome compared with patients who received the shorter course of chemotherapy. The 8-year relapse-free survival and overall survival were 87.8% and 87.5%, respectively, for patients receiving 15 months of chemotherapy.
Complications
Cardiomyopathy results primarily from anthracycline (doxorubicin) use. Patients should obtain routine follow-up echocardiograms after the completion of therapy.
Patients are at risk for renal failure because they have a single kidney.
Radiation effects have decreased but, in the past, have consisted of asymmetry of the muscle mass in the back.
Secondary malignant neoplasms may arise as a result of chemotherapy (particularly alkylating agents in combination with radiotherapy).
Infertility may occur as a result of the alkylating agents.
A risk of intestinal obstruction is noted.
Patient Education
Parents and patients must undergo formal chemotherapy instruction to learn about the adverse effects of medication. They must be encouraged to call with any questions and to become educated regarding the expectations of chemotherapy.
Parents must be taught regarding flushing schedules and how to maintain and care for the central venous catheter if it exits the skin and the procedure to follow if the patient develops a fever.
Patients who have undergone abdominal surgery are at risk for developing intestinal obstructions or scar tissue related to the surgery. Families must be educated to call when abdominal pain or vomiting develop that are not related to an infectious cause. All members of the pediatric oncology team also must have a heightened awareness of the risk of obstruction in these patients so that an abdominal radiograph is obtained if any suggestion of obstruction exists.
For excellent patient education resources, visit eMedicineHealth's Cancer Center. Also, see eMedicineHealth's patient education article Renal Cell Cancer.
-
Large right-sided heterogeneous renal mass in a 9-month-old infant. Biopsy findings were consistent with clear cell sarcoma of the kidney.
-
Recurrent clear cell sarcoma of the kidney occurring in a lymph node 18 months after therapy.







