Practice Essentials
Pneumomediastinum is an uncommon entity in pediatric practice. It is defined as free air or gas contained within the mediastinum, which almost invariably originates from the alveolar space or the conducting airways. The etiology of pneumomediastinum is multifactorial. [1]
Pneumomediastinum was first described by Laennec in 1819 as a consequence of traumatic injury. Spontaneous pneumomediastinum was reported in 1939 by Hamman, for whom the Hamman sign is named (see Physical Examination).
Many authors distinguish spontaneous pneumomediastinum as a form of pneumomediastinum that is not associated with blunt force or penetrating chest trauma, endobronchial or esophageal procedures, neonatal lung disease, mechanical ventilation, or chest surgery or other invasive procedures. Because of the infrequent occurrence of pneumomediastinum, the literature relating to pneumomediastinum involves individual case reports or small case series and is retrospective in nature.
The following images demonstrate radiographic findings in patients with pneumomediastinums.
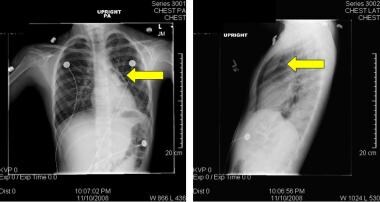
 This chest radiograph (posteroanterior and lateral view) is from a 3-year-old girl with a history of prematurity, chronic lung disease, and asthma who presented with a viral pneumonitis and persistent cough. On the posteroanterior view, a pneumomediastinum (arrow) is noted. Also, extensive subcutaneous air is observed.
This chest radiograph (posteroanterior and lateral view) is from a 3-year-old girl with a history of prematurity, chronic lung disease, and asthma who presented with a viral pneumonitis and persistent cough. On the posteroanterior view, a pneumomediastinum (arrow) is noted. Also, extensive subcutaneous air is observed.
 On the lateral radiograph from the patient in Media file 2, anterior mediastinal air is observed. Left lower lobe atelectasis is also present. The child was asymptomatic and was discharged 2 days later.
On the lateral radiograph from the patient in Media file 2, anterior mediastinal air is observed. Left lower lobe atelectasis is also present. The child was asymptomatic and was discharged 2 days later.
 Chest radiographs in anteroposterior (AP) and lateral projections obtained in a 9-year-old girl with wheezing and pneumonitis. The arrows highlight the "spinnaker sail sign" in which free mediastinal air lifts the thymus off of the heart and major vessels.
Chest radiographs in anteroposterior (AP) and lateral projections obtained in a 9-year-old girl with wheezing and pneumonitis. The arrows highlight the "spinnaker sail sign" in which free mediastinal air lifts the thymus off of the heart and major vessels.
Signs and symptoms
The following symptoms have been reported:
-
Chest pain
-
Dyspnea
-
Fever
-
Dysphonia
-
Throat pain
-
Jaw pain
-
Dysphagia
-
Neck swelling
-
Torticollis
See Presentation for more detail.
Diagnosis
Laboratory studies
The following laboratory studies are indicated in suspected cases of pneumomediastinum:
-
Arterial blood gas analysis
-
Cardiac enzymes
-
Toxicology
Imaging studies
Chest radiography usually (although not invariably) reveals a pneumomediastinum. Chest computed tomography (CT) may be used to diagnose pneumomediastinum not visualized on chest radiography. In addition, CT scanning may provide diagnostic information about the presence of coexisting illness, such as a perforated esophagus. Contrast studies have been recommended when esophageal perforation is suspected.
See Workup for more detail.
Management
Medical therapy depends on the clinical status of the patient. In general, most children with pneumomediastinum are asymptomatic, and the natural course is spontaneous resolution.
Surgical intervention is reserved for pneumomediastinum leading to marked cardiorespiratory compromise or circumstances of defined esophageal or tracheal tear.
See Treatment and Medication for more detail.
Pathophysiology
Pneumomediastinum rarely leads to clinically significant complications. More commonly, the associated or precipitating condition underlying pneumomediastinum may be the cause of significant illness. Rarely, tension pneumomediastinum has been reported in which elevated mediastinal pressure leads to diminished cardiac output because of direct cardiac compression or reduced venous return. When extensive subcutaneous and mediastinal gas is present, airway compression may also occur. Jennings et al (2013) report this as a complication following blunt thoracic trauma. [2]
The generally accepted explanation for the development of pneumomediastinum is that free air tracks from ruptured alveoli along peribronchial vascular sheaths toward the hilum of the lung. From there, it extends proximally within the mediastinum.
The Macklin effect, first described in 1939, highlights the sequence of events in the development of pneumomediastinum as follows: (1) alveolar rupture, (2) air dissection along the bronchovascular sheath, and (3) free air reaching the mediastinum.
The dissection of free air may not be confined solely to the mediastinum. Zylak et al note that the mediastinum communicates with the submandibular space, the retropharyngeal space, and vascular sheaths within the neck. [3] In addition, 2 routes of communication with the retroperitoneum have been noted: via a tissue plane extending through the sternocostal attachment to the diaphragm, as well as periaortic and periesophageal fascial planes. As a result, air present within the mediastinum may dissect through these tissue planes, causing pneumopericardium, pneumothorax, subcutaneous emphysema, pneumoperitoneum, or pneumoretroperitoneum.
Carolan et al report a case of spontaneous pneumomediastinum associated with the presence of air within the cervical and thoracic spinal canal indicative of air dissection from the mediastinum, neck, and back through soft-tissue planes and the neural foramina into the spinal canal. [4] They suggest use of the term “spontaneous pneumorrhachis” for patients with this finding. Behr et al (2018) note the finding of pneumorrhachis in 5.8% of a series of 241 patients with pneumomediastinum. [5] Pneumorrhachis was identified more frequently in patients in whom the distribution of air was seen in all three mediastinal compartments. Liu (2018) also notes that the presence of intraspinal air correlates with the severity and extent of spontaneous pneumomediastinum. Pneumorrhachis was also more common among subjects with spontaneous as opposed to secondary pneumomediastinum. [6]
In a study of 87 patients by Wong et al, the common causes of spontaneous pneumomediastinum included asthmatic exacerbation, infections (eg, pneumonia, lower respiratory tract infections), and choking. [7] In a narrative literature review, Gasser et al (2017) identifies asthma as a co-morbidity in 22% of patients with spontaneous pneumomediastinum. In this series, the most common triggering factors included bronchospasm (49%), cough (45%), vomiting (10%) and foreign body aspiration (8%). The cause or associated trigger was "idiopathic" in 33%. [8]
Etiology
A large and diverse group of factors has been implicated in the development of spontaneous pneumomediastinum. Various respiratory maneuvers that have in common the development of high intrathoracic pressures may lead to pneumomediastinum. These include Valsalva maneuvers, coughing, vigorous crying, and forceful retching or vomiting.
Elevated pulmonary (alveolar) pressures
Numerous maneuvers that lead to elevated alveolar pressures may result in pneumomediastinum (see discussion of the Macklin effect in Pathophysiology).
Forceful coughing, crying, or shouting may elevate pressures. Jones et al [9] report the development of spontaneous pneumomediastinum in a military training recruit after repeatedly shouting "Hooah!" during a motivational squad competition, highlighting that unique to the military training environment, vigorous shouting as a motivational stimulus can have barotraumatic consequences.
Vomiting, defecation, and Valsalva maneuver may elevate pulmonary alveolar pressures, as may illicit drug use, especially if associated with coughing.
Strenuous athletic activity, diving, flying, playing musical instruments, and childbirth are also potential risk factors. Sadarangani et al provide a case report of pneumomediastinum precipitated by weight lifting. [10] Improper breathing technique during weight lifting may increase the intrathoracic pressure and the risk of pneumomediastinum. The authors note the importance of physicians and trainers who work with athletes to provide instructions regarding proper breathing techniques during weight lifting.
Spirometry has been associated with the development of pneumomediastinum in 3 individual case reports.
Respiratory illness
Obstructive lung disease (eg, asthma, bronchiolitis, foreign body aspiration, bronchopulmonary dysplasia), especially in intubated and mechanically ventilated patients, is a risk factor.
Respiratory tract infections, especially if associated with asthma, may predispose a patient to the development of a pneumomediastinum. Fearon et al and Vazquez et al report cases in which pneumomediastinum is associated with mycoplasma lower respiratory tract infection. [11, 12] An association of severe spontaneous pneumomediastinum and laryngotracheitis in a young patient with asthma was reported by Lin et al, suggesting the need to consider spontaneous pneumomediastinum in the differential diagnosis of any patient presenting with cervical emphysema and signs of respiratory tract infection, especially in association with asthma. [13]
Hasegawa et al reported spontaneous pneumomediastinum complicating pneumonia in children infected with the 2009 pandemic influenza A (H1N1) virus. [14]
Spontaneous pneumomediastinum that is unrelated to positive pressure ventilation has been reported as a complication of severe COVID-19 pneumonia. [15, 16] Most cases resolve spontaneously with conservative management.
Foreign body aspiration has been reported in association with pneumomediastinum.
Organ injury
Penetrating or blunt injury to the thorax may cause air leak syndromes including pneumomediastinum. The etiology is thought to be related to the Macklin effect. Rezende-Neto et al reported that occult pneumomediastinum occurred in approximately 6% of all trauma patients with blunt chest injuries. [17] Patients with pneumomediastinum were more severely injured than those without as indexed by higher injury severity scores (ISS). However, none of the patients with occult pneumomediastinum had aerodigestive tract injuries and follow up chest CT scans demonstrated complete resolution of the pneumomediastinum in all cases.
Tracheobronchial rupture, esophageal injury, or perforation of a hollow abdominal viscus may lead to free mediastinal air.
Miscellaneous medical conditions
Pneumomediastinum has been reported in association with convulsions, tooth extraction, and dermatomyositis.
Epidemiology
United States statistics
The epidemiology of pneumomediastinum reflects that of the associated disease states, when present.
Spontaneous pneumomediastinum is an uncommon condition. A review by Chalumeau et al summarized the available literature. [18] Based on previous studies, they determined a prevalence of spontaneous pneumomediastinum ranging from 1 per 800 to 1 per 42,000 pediatric patients presenting to a hospital emergency department. Stack et al reported a 0.3% incidence of pneumomediastinum in association with asthma presenting to their institution over a 10-year period. [19] The mean age of affected patients was 11 years. No sex differences were observed in this cohort. Another study by Vianello et al that included 45 patients with severe acute asthma exacerbation found that 11.1% (five patients) were diagnosed with pneumomediastinum. [20]
A study from Nashville, Tennessee, reported the frequency of extra-abdominal gas in a series of patients undergoing laparoscopic esophageal surgery. Forty-seven percent of patients (N = 45) had evidence of extra-abdominal air on chest radiography. Of these, 86% had a pneumomediastinum. Pneumomediastinum persisted at least 1 postoperative day in two thirds of these cases. However, no mortality or morbidity was attributable to the presence of pneumomediastinum.
In a series of patients with sepsis-induced acute respiratory distress syndrome (ARDS), air leaks of any type, excluding pneumothorax, occurred in 3.7% of patients. [21] Ventilator pressures and volumes delivered were not correlated with the development of air leak.
In a series of adult patients presenting with blunt chest trauma, as many as 10% had evidence of pneumomediastinum. A study by Muckart et al that included 389 patients with blunt thoracic trauma reported a minimal incidence (5.9% for pneumomediastinum) of pneumomediastinum or pneumopericardium following blunt thoracic trauma. [22]
International statistics
A study by Briassoulis et al from Athens, Greece, evaluating the frequency of air leaks in children receiving mechanical ventilation reported a prevalence of 27%. [23] However, they did not report the prevalence of specific types of air leak.
Esayag et al reported an Israeli series of 13 patients with spontaneous pneumomediastinum. [24] This group represented 1 in 41,600 referrals to the emergency room and 1 in 15,500 hospitalizations. The median age of the patients was 19 years (range 2–72 y). Males comprised 77% of this group.
A case series from the Children's Medical Center, China Medical University in Taiwan reported by Lee et al defined an incidence of spontaneous pneumomediastinum in children of 1:8,302 patient visits to the pediatric emergency department. [25] They observed a bimodal distribution, with cases occurring in children younger than 4 years old and in adolescents aged 15-18 years. Males outnumbered females by a ratio of 4:1.
Sex- and age-related demographics
In a series of pneumomediastinum occurring in persons with asthma, there was a very slight male predominance in the prevalence of spontaneous pneumomediastinum. Other series confirm this excess of male cases. Damore and Dayan reported 29 cases of pneumomediastinum over a 10-year period unrelated to trauma, intubation, or surgical procedures; 69% of patients were male. [26] Some have suggested that a body habitus favoring a tall thin build is an additional risk factor for the development of spontaneous pneumomediastinum. The mechanisms underlying this association are unclear. Traumatic pneumomediastinum is more common in males, reflecting the male predominance among those who experience trauma and accidents.
The peak prevalence of spontaneous pneumomediastinum is seen in the second to fourth decades of life. This presumably reflects involvement in activities that increase the risk for developing pneumomediastinum, such as diving or marked physical exertion (eg, athletic activities, weight lifting). Moreover, the force of an individual's cough, vomit, and Valsalva maneuvers (all of which may lead to pneumomediastinum) attenuates with age, accounting for the decline in the prevalence of pneumomediastinum with age.
The age distribution for pneumomediastinum occurring in conjunction with specific disease processes reflects the age profile of the particular disease.
Prognosis
Although recurrent pneumomediastinum is a risk, the pneumomediastinum is almost invariably benign, with morbidity or mortality principally attributable to the associated or precipitating condition.
Morbidity/mortality
The mortality and morbidity associated with pneumomediastinum are generally attributable to underlying disease states. Spontaneous pneumomediastinum is usually a self-limited condition that rarely produces significant or life-threatening symptoms.
The mortality rate associated with pneumomediastinum may be as high as 50-70% as seen in Boerhaave syndrome (esophageal rupture following vomiting). The development of air leak, according to Weg et al, is not associated with an increased mortality rate in patients with sepsis-induced ARDS. [21] Other predisposing conditions associated with high mortality rates include trauma (blunt and penetrating, especially high velocity injury), asthma, and tracheobronchial perforation.
The most common morbidities attributable to pneumomediastinum are symptoms such as chest pain, voice change, and cough. Rarely, tension pneumomediastinum may result in decreased cardiac output. Laryngeal compression leading to stridor has been reported. Gas embolism has rarely been reported.
Complications
Associated air leaks
Other air leak syndromes (in particular, pneumothorax) may be observed in conjunction with pneumomediastinum.
Subcutaneous emphysema is commonly noted, although it is not usually associated with serious complications.
Tension pneumomediastinum
Although rare, tension pneumomediastinum may occur, leading to compression of the great veins, compromising venous return, which may result in hypotension and hypoxemia secondary to ventilation/perfusion mismatch.
Mediastinitis
Pneumomediastinum following massive vomiting may be associated with Boerhaave syndrome; developing mediastinitis is a risk.
Associated conditions
Complications may arise from associated conditions such as asthma, a foreign body, or drug ingestion.
Patient Education
Advise the patient to avoid high-risk activities. Instructions include the following:
-
Avoid strenuous athletic activities, particularly those involving Valsalva maneuvers such as weight lifting.
-
Avoid playing woodwind instruments.
-
Avoid barotrauma from activities such as flying, parachuting, or scuba diving.
-
Maintain good asthma control. Ensure that influenza and pertussis vaccinations are current.
-
Avoid smoking and inhalation of illicit drugs.
For patient education resources, see the Lungs Center, as well as Emphysema and Chest Pain.
-
This chest radiograph (posteroanterior and lateral view) is from a 3-year-old girl with a history of prematurity, chronic lung disease, and asthma who presented with a viral pneumonitis and persistent cough. On the posteroanterior view, a pneumomediastinum (arrow) is noted. Also, extensive subcutaneous air is observed.
-
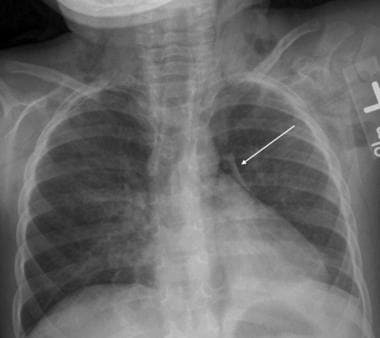
The chest radiograph is taken from an adolescent girl with status asthmaticus who was intubated for respiratory failure. A rim of air consistent with a pneumomediastinum may be observed along the upper left border of the heart. Subcutaneous air is observed in the soft tissues of the neck. She required very high peak inspiratory pressures (50 cm H2), which in conjunction with marked air trapping due to her asthma, caused alveolar rupture, allowing air to track to the mediastinum. A central venous line was placed.
-
On the lateral radiograph from the patient in Media file 2, anterior mediastinal air is observed. Left lower lobe atelectasis is also present. The child was asymptomatic and was discharged 2 days later.
-
Chest radiographs in anteroposterior (AP) and lateral projections obtained in a 9-year-old girl with wheezing and pneumonitis. The arrows highlight the "spinnaker sail sign" in which free mediastinal air lifts the thymus off of the heart and major vessels.
-
Subcutaneous emphysema and pneumothorax.






