Practice Essentials
Hypermagnesemia is defined as a serum concentration greater than 2.5 mg/dL. (The reference range of serum magnesium levels is 1.8-2.5 mg/dL.)
Signs and symptoms
Symptoms of hypermagnesemia are nonspecific at lower levels (2-4 mg/dL) and may include the following:
-
Nausea
-
Vomiting
-
Flushing
-
Lethargy
-
Weakness
-
Dizziness
Higher levels may lead to a depressed sensorium, and cardiopulmonary arrest may occur at extreme levels (>10-15 mg/dL).
See Presentation for more detail.
Diagnosis
Obtain blood urea nitrogen (BUN) and creatinine levels to determine the presence of renal insufficiency, as serum magnesium levels rise when the creatinine clearance is less than 30 mL/min.
Check creatine phosphokinase (CPK) or urine myoglobin in patients with suspected rhabdomyolysis.
Because hypothyroidism and adrenal insufficiency are rare causes of hypermagnesemia, perform thyroid function tests and at least an early morning serum cortisol test in recurrent or refractory cases of hypermagnesemia.
See Workup for more detail.
Management
Calcium chloride (5 mL of a 10% solution) may be administered intravenously over 30 seconds to directly antagonize the cardiac and neuromuscular effects of excess extracellular magnesium. Monitor these patients in an intensive care unit (ICU) setting and give careful attention to ECG parameters.
See Treatment and Medication for more detail.
Background
Magnesium is the second most abundant intracellular cation and the fourth most abundant cation overall. [1] Almost all enzymatic processes using phosphorus as an energy source require magnesium for activation. [2] Magnesium is involved in most biochemical reactions such as glycolysis and oxidative phosphorylation. Because magnesium is bound to adenosine triphosphate (ATP) inside the cell, shifts in intracellular magnesium concentration may help to regulate cellular bioenergetics. [3, 4, 5, 6]
Extracellularly, magnesium ions block neurosynaptic transmission by interfering with the release of acetylcholine. Magnesium ions also may interfere with the release of catecholamines from the adrenal medulla. In fact, magnesium has been proposed as being an endogenous endocrine modulator of the catecholamine component of the physiologic stress response.
Approximately 60% of total body magnesium is located in the bone, and the remainder is in the soft tissues. In this soft tissue intracellular compartment, which comprises about 38% of total body magnesium, relatively higher concentrations are found in the skeletal muscle and the liver. Because less than 2% is present in the extracellular fluid (ECF) compartment, serum levels do not necessarily reflect the status of total body stores of magnesium.
The reference range of serum concentration of magnesium is 1.8-2.5 mg/dL. Approximately one third of this magnesium is protein-bound. Analogous to plasma calcium, the free (ie, unbound) fraction of magnesium is the active component. Unfortunately, ionized serum magnesium cannot accurately be assessed at this time.
Less than 40% of dietary magnesium is absorbed; absorption takes place throughout the small intestine (predominantly in the ileum) and in the colon. A minimum daily intake of magnesium of 0.3 mEq/kg of body weight has been suggested to prevent deficiency. However, infants and children tend to have higher daily requirements of magnesium.
Elimination is predominantly renal; the threshold for urinary excretion nears the reference range of serum concentration. Thus, when serum levels are greater than 2.5 mg/dL, magnesium excretion dramatically increases. Conversely, the kidney retains a strong capacity to resorb magnesium, and the main site for reabsorption is the thick ascending loop of Henle.
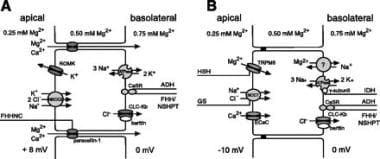 (A) Magnesium reabsorption in the thick ascending limb of the loop of Henle. The driving force for the reabsorption against a concentration gradient is a lumen-positive voltage gradient generated by the reabsorption of NaCl. FHHNC = Familial hypomagnesemia with hypercalciuria and nephrocalcinosis. ADH = autosomal dominant hypocalcemia. FHH/NSHPT = Familial hypomagnesemia/neonatal severe hyperparathyroidism. (B) Magnesium reabsorption in the distal convoluted tubule. Active transcellular transport is mediated by an apical entry through a magnesium channel and a basolateral exit, presumably via a Na+/Mg2+ exchange mechanism. HSH = Hypomagnesemia with secondary hypocalcemia. GS = Gitelman syndrome. IDH = Isolated dominant hypomagnesemia. Source: Konrad M, Schlingmann KP, Gudermann T: Insights into the molecular nature of magnesium homeostasis. Am J Physiol Renal Physiol 2004; 286: F599-F605.
(A) Magnesium reabsorption in the thick ascending limb of the loop of Henle. The driving force for the reabsorption against a concentration gradient is a lumen-positive voltage gradient generated by the reabsorption of NaCl. FHHNC = Familial hypomagnesemia with hypercalciuria and nephrocalcinosis. ADH = autosomal dominant hypocalcemia. FHH/NSHPT = Familial hypomagnesemia/neonatal severe hyperparathyroidism. (B) Magnesium reabsorption in the distal convoluted tubule. Active transcellular transport is mediated by an apical entry through a magnesium channel and a basolateral exit, presumably via a Na+/Mg2+ exchange mechanism. HSH = Hypomagnesemia with secondary hypocalcemia. GS = Gitelman syndrome. IDH = Isolated dominant hypomagnesemia. Source: Konrad M, Schlingmann KP, Gudermann T: Insights into the molecular nature of magnesium homeostasis. Am J Physiol Renal Physiol 2004; 286: F599-F605.
Renal reabsorption is impaired by several factors such as volume expansion, ethanol ingestion, hypercalcemia, and diuretic administration (eg, osmotic, thiazide, loop). Of these 3 types of diuretics, loop diuretics have a greater effect on renal magnesium wasting because of their site of action. [7]
Pathophysiology
Hypermagnesemia is defined as a serum concentration greater than 2.5 mg/dL. (The reference range of serum magnesium levels is 1.8-2.5 mg/dL.) Most cases of hypermagnesemia have been noted in patients with severe renal failure in whom magnesium intake has been excessive. This may result from iatrogenic administration of medications that contain magnesium. Fatal hypermagnesemia has resulted from the administration of enemas containing magnesium to patients with renal failure. In fact, hypermagnesemia is rarely observed in individuals with a glomerular filtration rate (GFR) that is within reference range. In patients with acute renal failure and hypermagnesemia, levels usually remain less than 4 mg/dL.
Araki et al reported the case of a 20-month-old girl with normal renal function who had received a usual dosage of magnesium oxide as a laxative and presented in a coma with hypermagnesemia (11.0 mg/dL). She recovered after administration of calcium gluconate infusion. [8]
Rapid mobilization of magnesium from soft tissues may result in hypermagnesemia following trauma, shock, cardiac arrest, or burns.
Hypermagnesemia usually occurs in individuals with significant diabetic ketoacidosis and often turns into hypomagnesemia during treatment. Thus, the initial hypermagnesemia is likely a pseudo-elevation secondary to dehydration, and the resulting hypomagnesemia may reflect intracellular shifting following insulin administration.
Neonates with hypermagnesemia whose mothers have received intravenous magnesium sulfate for pregnancy-induced hypertension may present with respiratory impairment, generalized hypotonia, and GI hypomotility mimicking intestinal obstruction. A retrospective study by Correia et al demonstrated that antenatal administration of magnesium sulfate is associated with high serum magnesium levels in neonates. [9] A study by Junqueira et al that included 251 preterm infants found that the presence of hypermagnesemia at birth was independently associated with early feeding intolerance. [10] Pregnancy in women who have congenital cardiac disease is associated with increased risk, but favorable outcomes occur in most cases. [11]
Etiology
Major predisposing factors for the development of hypermagnesemia include the following:
-
Renal failure (acute or chronic)
-
Iatrogenic over administration of magnesium (eg, antacids, cathartics)
-
Neonates born to mothers treated with magnesium sulfate for eclampsia
Epidemiology
United States statistics
Although the occurrence of hypermagnesemia has not been precisely defined, the disorder tends to occur in certain patient populations, particularly in patients with preexisting renal insufficiency.
Age-related demographics
Although no age predisposition to developing hypermagnesemia is noted per se, neonates whose mothers have been treated with magnesium sulfate for eclampsia may be born with significant elevations in serum magnesium concentration, which can range from 3-11 mg/dL.
-
(A) Magnesium reabsorption in the thick ascending limb of the loop of Henle. The driving force for the reabsorption against a concentration gradient is a lumen-positive voltage gradient generated by the reabsorption of NaCl. FHHNC = Familial hypomagnesemia with hypercalciuria and nephrocalcinosis. ADH = autosomal dominant hypocalcemia. FHH/NSHPT = Familial hypomagnesemia/neonatal severe hyperparathyroidism. (B) Magnesium reabsorption in the distal convoluted tubule. Active transcellular transport is mediated by an apical entry through a magnesium channel and a basolateral exit, presumably via a Na+/Mg2+ exchange mechanism. HSH = Hypomagnesemia with secondary hypocalcemia. GS = Gitelman syndrome. IDH = Isolated dominant hypomagnesemia. Source: Konrad M, Schlingmann KP, Gudermann T: Insights into the molecular nature of magnesium homeostasis. Am J Physiol Renal Physiol 2004; 286: F599-F605.




