Practice Essentials
Os odontoideum is an anatomic anomaly of the upper cervical spine that may be defined in radiologic terms as an oval or round ossicle with smooth circumferential cortical margins representing a hypoplastic dens (odontoid process) that has no continuity with the body of C2 (the axis). [1, 2]
In 1863, separation of the odontoid process from the body of the axis was first described in a postmortem specimen. In 1886, Giacomini coined the term os odontoideum for this condition. This entity is clinically important because a mobile or insufficient dens renders the transverse atlantal ligament (TAL) ineffective at restraining atlantoaxial motion. Translation of the atlas (C1) on the axis may compress the cervical cord or vertebral arteries. [3, 4]
Os odontoideum is rare, but the exact frequency is unknown. Many cases are incidentally detected. Others are diagnosed when patients become symptomatic. There are occasional reports of patients with os odontoideum becoming quadriparetic after minor trauma. [5, 6] To date, no large-scale screening studies have been performed. In one magnetic resonance imaging (MRI) study of odontoid morphology, a 0.7% (one case in 133 patients) incidence was reported. [7]
There are three evolving and controversial aspects of os odontoideum: etiology, surgical indications, and optimal management. The 2002 consensus report by Hadley et al called for several studies [8] :
-
Population-wide studies of the prevalence of os odontoideum as an incidental finding
-
A follow-up of incidentally noted and untreated os odontoideum, even with C1-2 subluxation.
-
A cooperative, multi-institutional natural history study of patients with os odontoideum without C1-C2 instability, to provide demographic and clinical factors predictive of the development of subsequent instability
-
A multi-institutional prospective, randomized trial comparing posterior wiring and fusion techniques with rigid C1-2 screw fixation
The age at diagnosis varies significantly from the first to the sixth decade of life. With increased awareness, however, os odontoideum has been diagnosed in younger patients. [9] The etiology remains controversial, but an increased frequency of os odontoideum has been reported in patients with Morquio syndrome, [10, 11] multiple epiphyseal dysplasia, and Down syndrome.
There are two main forms of management:
-
Clinical and radiologic surveillance
-
Operative stabilization
Surgical stabilization may be recommended in the following three settings:
-
Spinal instability
-
Neurologic involvement
-
Intractable pain
Anatomy
Successful treatment of os odontoideum requires an understanding of the unique anatomic characteristics of the cervicocranium (occiput-C2). The bony elements here develop through enchondral ossification.
The tip of the dens and its associated ligaments arise from the fourth occipital through the cervical-0 (C0) somites, which do not ossify until middle childhood. [12, 13] The base of the dens forms from the C0 and C1 sclerotomes as two paired structures that ossify just before birth. The C2 and C3 sclerotomes give rise to the body of the axis, which fuses with the dens at age 4 years. (See the image below.)
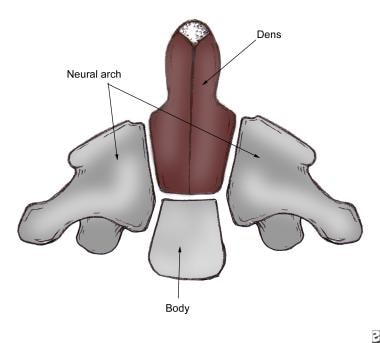 The axis has 5 primary and 2 secondary ossification centers. C0, C1, and C2 sclerotomes contribute to various portions of the dens. The principal portion of the dens body arises from the original center of C1.
The axis has 5 primary and 2 secondary ossification centers. C0, C1, and C2 sclerotomes contribute to various portions of the dens. The principal portion of the dens body arises from the original center of C1.
In a study of human embryos at 8 weeks' gestation, O’Rahilly et al reported that no transverse segmentation formed within the odontoid process at any time. An embryologic anomaly characterized by a complete/partial segmentation of two rostral parts will result in a bipartite dens rather than an os odontoideum. [14]
The atlantoaxial joint (C1-2) consists of biconcave articulations with loose capsules and small contact areas. Stability is therefore conferred by associated ligaments, including the TAL, which is the primary restraint to flexion and extension. A study of 41 patients with irreducible os odontoideum found that the position of the TAL anterior and inferior to the ossicle was the most common factor associated with irreducibility. [15]
Other important restraints include the apical ligaments, the alar ligaments, the tectorial membrane, and the atlanto-occipital membranes
The vertebral arteries are intricately invested in the bony anatomy of the atlantoaxial segment. They pass just inferior to the C1-2 facet joint, then course laterally through the transverse foramen of C2. Just above the C1 lateral mass, they turn medially and meet to progress cephalad into the foramen magnum. [16] Aberrancy of the vertebral artery course is not rare and may limit fixation options in some patients selected for operative management of os odontoideum. This deviant course may be unilateral or bilateral.
Pathophysiology
Initially, os odontoideum was thought to represent a congenital failure of fusion of the dens to the remainder of the axis. As such, the condition is usually grouped with other craniocervical junction abnormalities, such as dental aplasia and hypoplasia. [17, 18, 19, 20, 21, 22, 23, 24] Today, it seems clear that failure of the secondary ossification center of the dens to fuse with the base of the odontoid represents a separate entity known as persistent ossiculum terminale. [25]
Differentiation between os odontoideum and persistent ossiculum terminale is clinically critical. The ossicle of the ossiculum terminale is much smaller than that of the os odontoideum. More important, that ossicle lies at the level of the atlantal ring above the transverse atlantal ligament. In this cranial location, ossiculum terminale, unlike os odontoideum, is not associated with significant instability.
Some authors speculate that os odontoideum represents a previous fracture of the odontoid synchondrosis before its closure at age 5-6 years. [26, 27, 28, 29] These authors describe os odontoideum in patients with previously normal cervical radiographs. For example, Schuler et al elegantly described the evolution of an os odontoideum following trauma in a child. [30] Subsequently, Menezes identified os odontoideum in children younger than 5 years with a previously normal odontoid. He associated the os with unrecognized fractures. [31]
In this model, os odontoideum develops gradually. Following a fracture of the odontoid synchondrosis, with growth, the alar ligaments carry the dens fragment away from the axis base. The cranial portion of the dens fragment continues to receive a blood supply from the vascular arcade. The avascular caudad portion resorbs, leaving the characteristic rounded ossicle.
One paper documented os odontoideum formation after a fracture with serial radiographs. [32] Another report, in a 4-year-old girl, showed an incompletely ossified, cartilaginous orthotopic os. [33] The authors argued for a multifactorial etiology related to the embryology and vascular supply of the odontoid process. A case from the year before made a similar argument with a posttrauma computed tomography (CT) scan showing no fracture, followed by os odontoideum 10 years later. [34]
Authors who favor a congenital basis for os odontoideum point out that the craniovertebral junction is one of the most common sites for malformation. Included are clefts or aplasia of anterior and posterior arches of atlas. [17, 20, 21, 28] On the other hand, unlike most congenital malformations, os odontoideum tends to occur as an isolated entity without other regional anomalies. Garg et al reported a case of os odontoideum in a myelopathic 16-year-old patient with bipartite atlas. [35] They concluded that the coexistence of these conditions supports the embryologic basis for os odontoideum. In this case, the dens had an “unusual bony projection” on its anterior surface.
Crockard and Stevens reviewed the embryologic and comparative anatomy data of clinical syndromes associated with craniocervical instability. [36] They concluded that os odontoideum is the product of excessive movement at the time of ossification of the cartilaginous dens and is analogous to the unfused type II odontoid fracture. True hypoplasia of the odontoid peg, on the other hand, was found to be part of a wider segmentation defect associated with Klippel-Feil syndrome, [37] occipitalized atlas, or basilar invagination and rarely was found to be associated with instability.
In 2006, Sankar et al reviewed 519 consecutive patients with radiographic abnormalities in the occipitocervical region. [38] Os odontoideum was confirmed in 16. Only three of those patients had a history of remote trauma. The authors concluded that this supported an embryologic basis for the condition.
The size of the os odontoideum may vary, but it typically is smaller than the normal dens, particularly at its base. Perhaps there are two etiologic groups. Certainly, in patients with other congenital anomalies or odontoid malformations, an embryologic basis may be assumed. Unfortunately, individual correlations do not prove the case one way or the other. A report of three cases of familial os odontoideum was published in 2011. [39]
Regardless of the underlying cause, sound treatment selection requires an understanding of the natural history of this process. It is known that in a subset of patients, the secondary ligamentous restraints become lax. With increasing laxity, anterior motion of the atlas on the axis can become excessive. When the instability has been longstanding, it becomes multidirectional. Less clear are the percentages and rates of progression to instability. Because no population studies are available, assumptions are made on the basis of case series data from nonoperatively managed patients.
Two types of os odontoideum are described, according to the position of the dens tip: orthotopic and dystopic. In orthotopic os odontoideum, the dens fragment lies in an anatomic position. In dystopic os odontoideum, the dens tip is in any other position. Most commonly, the fragment is located near the foramen magnum, where it may fuse with the clivus. Alternatively, the os may be fixed to the anterior ring of the atlas.
Subluxation and instability are described in both types of os odontoideum. Some authors believe that dystopic os odontoideum is more likely to be symptomatic.
In years to come, both posttraumatic and congenital forms of os odontoideum may be identified; however, authors in each camp have often written as if their hypothesis has been all but proved. Understanding the true etiology of this disorder may be helpful in terms of identifying high-risk patients through genetic testing.
If os odontoideum is posttraumatic, the increased use of advanced imaging modalities such as spiral CT and MRI may markedly decrease its incidence in the future. Furthermore, better explication of the etiology may better delineate progression risk, leading to decreased x-ray exposure during follow-up and the limiting of operative intervention only to those patients at high risk for progression. These data may also support or eliminate the need for activity restriction during the observation phase.
Prognosis
Outcomes and prognosis data for os odontoideum patients have been limited to scattered case reports and small case series. These series have typically described successful outcomes with both nonoperative and surgical management. [40, 41, 42]
Klimo et al investigated 77 patients with os odontoideum who underwent surgical stabilization. [3] In all patients, fusion was achieved at a mean duration of 4.8 months. It was reported that 90% of patients experienced improvement in their neck pain or neurologic symptoms. Furthermore, it was reported that 39% of the patients who presented with myelopathy had complete resolution, 50% showed improvement in their spasticity, and 11% had constant and unchanged spasticity.
Spierings et al described their management of 37 os odontoideum patients. [43] At a median follow-up of 7 years, of the 16 with neck pain only, none developed neurologic deficits. Four patients had mild or transient myelopathy and limited radiographic instability and were also followed nonoperatively. With a maximum follow-up of 14 years, three of the four had no recurrence; one had stable monoparesis. Seventeen patients with myelopathy and more instability underwent surgery. The authors found no difference in neck pain between the surgical and nonsurgical groups.
In a series by Dai et al, five patients with os odontoideum without symptoms were treated nonoperatively and were monitored for an average of 6.5 years. [44] None of these patients reported symptom progression during the follow-up period.
In a study of 35 os odontoideum patients, Fielding et al found that 27 were radiographically unstable. [45] Of those 27, 26 underwent successful Gallie fusion. The authors reported “solid” fusions after 2 months of immobilization in children and 3 months in adults. The 27th unstable patient refused surgery and remained well at 2-year follow-up examination. The eight stable patients were managed nonoperatively and remained well at last follow-up. Symptomatically, two thirds of the 35 patients studied had only mechanical pain. These patients reported resolution after fusion.
The neurologic outcome in patients with symptomatic cord compression is less clear. After surgery, symptomatic progression typically ceases, and most patients report significant symptomatic improvement. These patients can be divided into those with acute incomplete cord syndromes and those with more insidious myelopathic syndromes. Typically, transient neurologic signs following trauma are associated with a good prognosis. Rapid functional return parallels improvement in neurologic signs, and recurrence rates are low.
A retrospective study of 21 patients treated with rigid posterior instrumentation showed a mean improvement in the Nurick scale for myelopathy of 2.3 before surgery to 0.7 at the time of follow-up. [46] At a mean 34.7 months of follow-up, Odom's criteria outcomes were excellent in 47%, good in 37%, fair in 11%, and poor in 5%. All patients with preoperative neck pain had symptom relief or improvement, with all of these patients having more than 83.7% improvement in visual analogue scale (VAS) scores. The authors reported a mean improvement in space available for the cord (SAC), from 9.3 mm to 17.7 mm. There were no pseudarthroses or screw failures.
Zhang et al determined that patients with asymptomatic or myelopathic atlantoaxial instability secondary to os odontoideum were at risk for acute spinal cord injury after minor traumatic injury. [47] They suggested that fixation and fusion should be undertaken as prophylactic treatment to avoid these injuries.
Patients with cerebellar or medullary signs exhibit a more progressive course. In that these patients gradually worsen, surgery is most clearly indicated in this setting.
In a retrospective multicenter review, Saarinen et al compared the outcomes of conservative (n = 10) and surgical treatment (n = 34) of idiopathic os odontoideum in children with the outcomes of conservative (n = 10) and surgical treatment (n = 34) of nonidiopathic os odontoideum. [48] The authors found that patients with idiopathic os odontoideum who had a stable atlantoaxial joint at presentation remained asymptomatic and intact during conservative treatment. Children with idiopathic os odontoideum who underwent spinal arthrodesis had significantly lower complication and nonunion rates than children with nonidiopathic os odontoideum.
-
The axis has 5 primary and 2 secondary ossification centers. C0, C1, and C2 sclerotomes contribute to various portions of the dens. The principal portion of the dens body arises from the original center of C1.
-
A coronal reconstruction of an orthotopic os odontoideum. Note the wide gap between the rounded ossicle and the base of the axis.
-
A sagittal reconstruction of a CT scan demonstrating a dystopic os odontoideum. Note that the ossicle appears fused to the clivus (anterior portion of the foramen magnum). Also note the smooth corticated border of the ossicle.
-
Anterior-posterior tomogram view of a type II dens fracture. The fracture line is narrow and lower on the waist of the dens, unlike the fracture line of an os odontoideum. No cortication is noted along the fracture line.
-
Flexion lateral radiograph of a dystopic displaced os odontoideum. Note the limited posterior interval between the dens and the posterior C1 ring (PADI). This patient had reported electric shocks radiating down the body (ie, Lhermitte sign), as well as progressive weakness and ataxia.
-
Extension lateral radiograph of a dystopic displaced os odontoideum. This deformity did not reduce with extension.
-
T2-weighted parasagittal MRI image of a patient with os odontoideum and mild compression of the upper cervical spine. This patient presented with transient quadriparesis.
-
Lateral radiograph of a dystopic displaced os odontoideum 6 months after posterior wiring. After the wiring was performed, the patient had a solid arthrodesis with no motion on flexion and extension. Her neurologic symptoms resolved despite the failure to obtain a reduction. Had she continued to have severe symptoms, anterior odontoidectomy could have been considered.
-
Lateral radiograph demonstrating fixation of a reduced os odontoideum with Magerl screws in a patient with an incomplete posterior arch of C1.
-
Lateral radiograph demonstrating fixation of a reduced os odontoideum with the Harms technique.




