Background
Ocular cicatricial pemphigoid (OCP) is one of the subsets of mucous membrane pemphigoid (MMP), a group of systemic autoimmune diseases characterized by T-lymphocyte dysregulation, the production of circulating autoantibodies directed against a variety of adhesion molecules in the hemidesmosome-epithelial membrane complex, and the production of proinflammatory cytokines and immune system activation markers. OCP can affect the skin and other mucous membranes (eg, oral mucosa, pharynx, larynx, trachea, esophagus, vagina, urethra, anus), in addition to its hallmark feature, chronic cicatrizing conjunctivitis. [1]
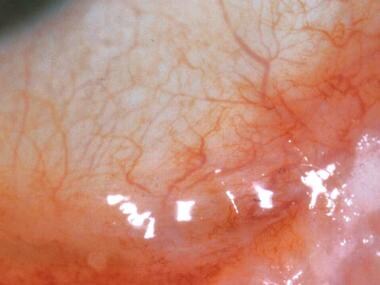
See image below depicting stage II ocular cicatricial pemphigold.
Pathophysiology
The pathophysiologic mechanisms of ocular cicatricial pemphigoid (OCP), as well as conjunctival fibrosis, are not completely understood. Clearly, a defect exists in immunoregulation, with the production of autoantibodies directed against the beta 4 subunit of alpha 6 beta 4 integrin, and, reportedly, in some instances, against alpha 3, beta 3, or gamma 2 subunits of laminin 5. [2]
A triggering agent in the genetically susceptible individual, leading to clinical manifestations of the disease, may occur in a "2-hit" mechanism. It is probably operative in some patients. Human leukocyte antigen DR2 (HLA-DR2), human leukocyte antigen DR4 (HLA-DR4 [HLA-DR*0401]), and human leukocyte antigen DQw7 (HLA-DQw7 [DQB1*0301]) genotypes have been identified as conferring increased susceptibility to the development of OCP.
In some patients, systemic practolol therapy and topical antiglaucoma drugs, such as pilocarpine, timolol, epinephrine, Humorsol, idoxuridine, and phospholine iodide, have triggered the onset of OCP. The term pseudopemphigoid or drug-induced pemphigoid may be used to describe these cases. Whether or not these cases associated with medication use are identical to OCP is not completely clear.
On the molecular level, the initial trigger may be a process by which the OCP antigen undergoes a conformational change that provides antigenic stimulation. This signal results in the generation of B-cell clones that produce antibodies against antigens located at the basement membrane zone (BMZ), initiating a type II Gell and Coombs hypersensitivity reaction. The antibodies of immunoglobulin G (IgG), immunoglobulin A (IgA), and/or immunoglobulin M (IgM) bind to the antigen and initiate complement activation.
Circulating autoantibodies are difficult to demonstrate by classic indirect immunofluorescence technique in patients with OCP. Specialized radioimmunoassay and immunoblot techniques allow the circulating autoantibodies to be seen in all patients with OCP who have active conjunctivitis. The resultant inflammatory mediators that are produced induce migration of lymphocytes, eosinophils, neutrophils, and mast cells to the BMZ. The separation of the epithelium from the underlying tissues within the BMZ may be the result of direct cytotoxic action or the effect of lysosomal proteolytic enzymes.
Fibroblast activation secondary to inflammatory cytokine influences, with collagen production and subsequent cicatrization, is the end result in the conjunctiva. Progressive fibrosis causes profound tear insufficiency, meibomian gland dysfunction, and mucin deficiency. Symblepharon formation, trichiasis, distichiasis, and keratinization cause corneal epitheliopathy, persistent corneal epithelial defects, stromal ulcers, corneal scarring, neovascularization, and even perforation.
OCP is a chronic, slowly progressive, bilateral blinding, systemic autoimmune disease. Multiple antigens in the BMZ of squamous epithelia may serve as targets for a spectrum of autoantibodies observed in OCP. The molecular definition of these autoantigens facilitates the classification and characterization of subsets of OCP. Sera from patients with OCP have been shown to recognize beta 4 integrin, which is a 205-kDa protein, also known as CD104. A subset of patients with clinical features similar to OCP also has been shown to have autoantibodies against epiligrin, which is identified as laminin 5, a ligand for alpha 6 beta 4 integrin, and autoantibodies to the alpha 6 integrin subunit. OCP probably is a spectrum of several different diseases associated with different target antigens, different triggers, and different therapeutic responses.
Epidemiology
Frequency
United States
The incidence of ocular cicatricial pemphigoid (OCP) is estimated at between 1 in 8,000 and 1 in 46,000 ophthalmic patients. It is likely that the early stages of OCP are not reflected in these estimates because of difficulties in making the correct diagnosis. The real frequency of the disease is probably higher.
International
Distribution appears to be worldwide. No geographic predilection is reported.
Mortality/Morbidity
Oral lesions occur in 75-100% of patients with OCP. Skin involvement (eg, face, neck, scalp) occurs in approximately 25% of patients with OCP.
Race
OCP can occur in all races.
Sex
Females predominate patients diagnosed with OCP. The female-to-male ratio is estimated to be 1.5:1 to 3:1.
Age
Average age of onset is 50-60 years; however, the exact age of onset may be younger, since most patients with early stages of OCP remain undiagnosed. Some cases have been diagnosed as early as 12 and 19 years.
Prognosis
Based on the results of one study, slightly more than one third of patients with ocular cicatricial pemphigoid (OCP) receiving immunosuppressive therapy, according to the guidelines for use of immunosuppressive agents, respond to the therapy and remain free of inflammation following the cessation of therapy. Another one third of patients were free of disease activity, but they continued to receive chemotherapy because their disease had been controlled for only a short time (< 1 y) or because they had a history of relapse while on therapy. Nearly one third of patients only responded partially to treatment. Inability to control inflammation and to stop progression of cicatrizing conjunctivitis was seen only in a few individuals. In these patients, intravenous immunoglobulin seems to be effective. [3]
Patient Education
Patients with ocular cicatricial pemphigoid (OCP) should be educated about the disease, the potential consequences, and the therapy. It is a systemic disease affecting the eye; therefore, no topical medication can be curative.
It should be explained to patients that chemotherapy is currently the only available effective treatment of OCP, providing its safety by regular monitoring by an oncologist, rheumatologist, or other specialist familiar with immunosuppressive therapy. [4]
-
Ocular cicatricial pemphigoid, stage II. Note the fornix foreshortening.
-
Ocular cicatricial pemphigoid, stage III. Note the symblepharon.
-
Ocular cicatricial pemphigoid, stage IV. Note the ankyloblepharon and ocular surface keratinization.
-
Corneal neovascularization with ulceration and stromal thinning after persistent epithelial defect in a patient with ocular cicatricial pemphigoid.




