Background
Field defects typical of ischemic optic neuropathy were probably first described by Knapp in 1875. Miller and Smith first used the term ischemic optic neuropathy in 1966, and Hayreh later added the term anterior. In 1924, Uhthoff first described severe visual loss, with field defects and swollen optic discs. [1]
Anterior ischemic optic neuropathy (AION) is the most common cause of acute optic neuropathy in older age groups. It may be nonarteritic (nonarteritic anterior ischemic optic neuropathy [NAION]) or arteritic (AAION), the latter being associated with giant cell arteritis (GCA; often termed temporal arteritis). AION is characterized by visual loss associated with optic disc swelling of a pallid nature, sometimes with flame hemorrhages on the swollen disc or nearby neuroretinal layer, and sometimes with nearby cotton-wool exudates. Visual loss is usually sudden or develops over a few days at most and is commonly unilateral, although second eye involvement may occur later, especially in the arteritic form. The visual loss is usually permanent, with some recovery possibly occurring within the first weeks or months. Optic atrophy of varying degrees ensues within the next few weeks as a result of the hypoxic episode and is usually generalized but may be sectorial in NAION.
Although the pathophysiology differs in the arteritic form of AION, optic nerve ischemia is the common causative factor of both the acute episode and the resultant visual loss.. According to Rucker, temporal arteritis probably was first described a millennium ago by Ali Ibn Isa (AD 940-1010). [2] In modern times (1890), Hutchinson described a disease of this nature, and, in 1932, Horton and colleagues at the Mayo Clinic used the term temporal arteritis. [3, 4] To better describe the histologic features, Gilmour suggested the term giant cell arteritis in 1941. As a result of understanding that the mechanism for GCA was inflammatory and often not merely localized to optic nerve ischemia, treatment of GCA with steroids was started at the Mayo Clinic in 1949.
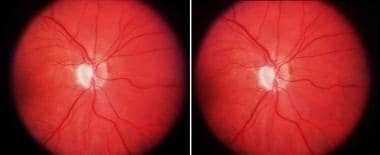
 Anterior ischemic optic neuropathy of the right eye. Swollen pale disc that can be seen in a stereoscopic view by converging the eyes and fusing the central image.
Anterior ischemic optic neuropathy of the right eye. Swollen pale disc that can be seen in a stereoscopic view by converging the eyes and fusing the central image.
 Sectorial optic atrophy of the right eye as a late finding resulting from anterior ischemic optic neuropathy. Atrophy has supervened, and the atrophic pale disc with a more pronounced cup can be seen steroscopically.
Sectorial optic atrophy of the right eye as a late finding resulting from anterior ischemic optic neuropathy. Atrophy has supervened, and the atrophic pale disc with a more pronounced cup can be seen steroscopically.
Pathophysiology
Anterior ischemic optic neuropathy (AION) is thought to be an ischemic process affecting the posterior circulation of the globe, principally vessels (ie, short posterior ciliary arteries) supplying the optic nerve at its exit from the eye. Only glial cells support the optic disc at this site, and it is the only portion of the optic nerve in which swelling can occur. More posterior ischemia results in a similar condition, without visible swelling, and is termed posterior ischemic optic neuropathy.
Early observations of optic disc photographs suggested that patients with congenitally smaller discs and having smaller or nonexistent optic nerve cups have an anatomical predisposition for nonarteritic anterior ischemic optic neuropathy (NAION). As an ischemic episode evolves, the swelling compromises circulation within a presumable already more compact disc, with a spiral of ischemia and swelling resulting in further neuronal damage. This type of structural/ischemic spiral is less implicated in the arteritic type of AION, in which the entire ophthalmic arterial circulation to the eye and orbit may be compromised.
Epidemiology
Frequency
United States
Patients with both arteritic and nonarteritic forms of anterior ischemic optic neuropathy (AION) are usually older than 50 years, with females predominating in the arteritic group. The incidence of nonarteritic anterior ischemic optic neuropathy (NAION) is 2.3-10.3 per 100,000 in the United States, and, for the arteritic type, it is 0.36 per 100,000. In the arteritic group, the incidence increases almost exponentially with advanced age. The literature seems to support the notion that whites are affected more commonly than blacks in the nonarteritic group, and people of Scandinavian or European ancestry are the most commonly affected ethnic group in the arteritic type.
International
In the nonarteritic group, incidence is higher in whites and uncommon in other races. The countries with the highest incidence of arteritic AION are the Scandinavian countries (ie, Norway, Denmark, Sweden, Finland), followed by Germany. The arteritic form occurs less frequently in non-Caucasians. Whether this racial discrepancy is genetic or due to medical care issues remains to be discovered.
Mortality/Morbidity
Although NAION may be associated with conditions such as hypertension, diabetes, and myocardial infarction, many individuals with NAION do not have such life-threatening vascular diseases. The role of smoking in this disease is unclear. By contrast, the arteritic form of AION has significantly more nonocular morbidity since it is associated with giant cell (cranial) arteritis. This condition affects the arterial vascular supply of many organs of the body, and the incidence of death associated with it is higher than that of the general population. Late-onset abdominal aortic aneurysms contribute to the morbidity and mortality of giant cell arteritis (GCA).
Bilateral visual loss is more common in the arteritic form of the disease, especially if treatment is delayed, and approximates 50% in some earlier series. By contrast, bilateral visual loss may be seen in 12-19% of nonarteritic anterior ischemic optic neuropathy (NAION), and it usually occurs more sequentially instead of almost simultaneously.
Progressive visual loss in the contralateral eye can occur in either form of AION, despite steroids, anticoagulation, or hyperbaric oxygen. Progressive visual loss is less common and usually stabilizes in a few days.
Race
Nonarteritic anterior ischemic optic neuropathy (NAION) is most common in whites (95%); it is less common in blacks (2%), Asians (3%), and Hispanics (1%). The arteritic form of the disease is predominantly described among whites of European descent, particularly Scandinavian and German.
A past misconception was that black patients did not succumb to GCA. However, numerous documented cases of GCA in blacks are noted; GCA in black patients is not uncommon.
Sex
Females dominate the incidence in both forms of AION, but only slightly in the nonarteritic form (1.2:1) compared with the arteritic type (2:1).
Age
Both disorders are found in older age groups. In the nonarteritic group, age ranges from the late 40s and older. The arteritic group almost always is older than 50 years, with an exponential increase with advanced age (90% of patients are >60 y). Rare cases of AION occur before 40 years, and the differentiation from optic neuritis associated with demyelinating disease is important in this crossover age group.
-
Anterior ischemic optic neuropathy of the right eye. Swollen pale disc that can be seen in a stereoscopic view by converging the eyes and fusing the central image.
-
Sectorial optic atrophy of the right eye as a late finding resulting from anterior ischemic optic neuropathy. Atrophy has supervened, and the atrophic pale disc with a more pronounced cup can be seen steroscopically.






