Practice Essentials
Ureteral injury is one of the most serious complications of gynecologic surgery. Less common than injuries to the bladder or rectum, ureteral injuries are far more serious and troublesome and when unrecognized are often associated with significant morbidity. Complications of unrecognized ureteral injuries include ureterovaginal fistulas, ureteral obstruction with potential loss of kidney function, formation of pelvic fluid or abscess collection, and sepsis. [1] For those reasons, injuries to the urinary tract, particularly the ureter, are the most common cause for legal action against gynecologic surgeons.
Therefore when a ureteral injury does occur, quick recognition of the problem and a working knowledge of its location and treatment are essential in providing patients with optimal medical care. The purpose of this article is to elucidate how and why ureteral injuries occur and to review their surgical and nonsurgical treatments.
History of the Procedure
Berard (1841) and Simon (1869) reported the earliest recorded repairs of ureteral injuries in gynecologic surgery. While the exact details of this procedure are unknown, the ureter and its course were poorly understood. In the early 1900s, Dr John Sampson, then a young faculty member at Johns Hopkins University, conducted the first systematic study of the ureter. During the next 100 years, as the surgical management for gynecologic disease progressed, many contributions were made to the understanding of the etiology, prevention, diagnosis, and treatment of iatrogenic ureteral injuries.
Problem
A significant ureteral injury is defined as any recognized or unrecognized iatrogenic trauma to the ureter that prevents it from functioning properly or effectively. The injury may lead to acute ureteral obstruction (ie, inadvertent ligation or kinking), discontinuity (ie, ureteral transection), or delayed/chronic ureteral obstruction (ie, ureteral devascularization and ischemia).
Epidemiology
Frequency
The frequency of ureteral injury following gynecologic surgery historically has been reported at approximately 1%. Ureteral injury can occur with oophorectomy, hysterectomy from any approach, pelvic organ prolapse repair (ie, cystocele with uterosacral ligament suspension), and even has been described as an extremely rare complication of transvaginal oocyte retrieval for in vitro fertilization. [2] Incidence rates of ureteral injury in gynecologic procedures are as follows [3] :
-
Emergency cesarean delivery: 0.01-0.06%
-
Vaginal hysterectomy: 0.02-0.5%
-
Abdominal hysterectomy: 0.03-2.0%
-
Laparoscopic hysterectomy: 0.13-6.0%
-
Urogynecologic procedures (anti-incontinence/prolapse): 1.7-4.3%
Despite the very low incidence of ureteral injury, prevention and detection is critical to the overall outcome. Several studies have examined the use of ureteral catheters on the impact on of ureteral injury. One systematic review identified six studies of ureteral catheterization in minimally invasive gynecologic surgery and found no indication that placement of ureteral catheters reduces the rate of ureteral injury, but did find an indication that it may increase morbidity. [4] In contrast, another systematic review that included five studies of laparoscopic gynecologic surgery concluded that prophylactic ureteral catheter placement can reduce the rate of ureteral injury, as well as shorten operative time and reduce the amount of bleeding. [5]
European Association of Urology guidelines recommend the use of preoperative placement of ureteral stents in high-risk cases, noting that although prophylactic stenting is not associated with a decrease in the likelihood of ureteric injury, it probably eases the intraoperative detection of ureteral injury. [3]
Cystoscopy is routinely used in surgery for pelvic organ prolapse and at the time of hysterectomy in order to detect urinary tract injury. A systematic review of 79 studies of gynecologic surgery for benign conditions found an adjusted ureteric injury rate of 0.3%. The authors concluded that routine intraoperative cystoscopy may improve detection of injuries intraoperatively but does not impact postoperative recognition. [6] Multiple studies have shown clear benefit of the use of cystoscopy for detection of ureteral obstruction for pelvic organ prolapse surgeries.
Because intraoperative recognition of ureteral injury may be difficult, a high postoperative index of suspicion and detection is critical for prompt management and prevention of more significant sequelae.
Hysterectomy
The rate of ureteral injuries during hysterectomy varies but is consistently low across all surgical approaches. Some, but not all, studies have found that rates are higher with laparoscopic than with open hysterectomy. In the 2004 eVALuate study, which consisted of parallel randomized trials, rates of ureteral injury with laparoscopic procedures were 0.7% for abdominal hysterectomy and 0.3% for vaginal hysterectomy; no ureteral injuries occurred with open procedures. Overall, however, the authors concluded that despite the higher rate of ureteral injury, the benefits of the laparoscopic approach (eg, less pain, shorter hospital stay) outweighed the potential risks. [7]
A 2014 systematic review determined the risk of ureteral injury during laparoscopic hysterectomy to be 0.02%-0.4%. These investigators concluded that, contrary to earlier published findings citing high urinary tract injury rates, laparoscopic hysterectomy was a safe procedure in terms of the ureter. [8] However, a 2023 meta-analysis reported a higher incidence of ureteral injuries with laparoscopic versus open hysterectomy (pooled odds ratio [OR] 2.12, 95% confidence interval [CI] 1.71-2.62). [9]
A review of a California inpatient database for 2007 to 2011 by Blackwell et al found that ureteral injury occurred in 1753 of 223,872 patients (0.78%) undergoing hysterectomy and was unrecognized in 1094 (62.4%). The 90-day readmission rate increased from a baseline of 5.7% to 13.4% after recognized injury and 67.3% after unrecognized injury. Ureteral injuries independently increased the risk of sepsis and urinary fistula, while unrecognized ureteral injury increased the odds of acute kidney insufficiency and death. [10]
A review of 45,139 patients who underwent hysterectomy for benign gynecologic indications found that the incidence of any lower urinary tract complication was 0.2%; ureteral obstruction was the most commonly reported complication, accounting for 0.1% of cases; ureteral fistulae comprised 0.07% of cases. Factors significantly associated with the occurrence of any lower urinary tract complication recognized in the first 30 days postoperatively were endometriosis (adjusted odds ratio [OR] 2.29), Black race (adjusted OR 1.90), and prior abdominal surgery (adjusted OR 1.53). [11]
A systematic review reported that regardless of the surgical approach, rates of ureteral injury were significantly higher in women undergoing hysterectomy for malignancy. [12] For benign versus malignant histology, rates of ureteral injury were as follows:
-
Open abdominal hysterectomy: 255 vs 577 events per 100,000 cases
-
Laparoscopic hysterectomy: 262 vs 814 events per 100,000 cases
Cesarean delivery
A systematic review of 96 studies of iatrogenic bladder and ureter injuries that included 1.7 million women found that in cesarean delivery, the weighted pooled rate of ureteric injuries was nine per 100,000 procedures. [12]
Pelvic organ prolapse repair
Ureteral injury rates for treatment of pelvic organ prolapse are estimated to be 0.3% to 11%. Ureteral injury in this setting is likely related to the inability to identify the ureteral course in vaginal surgery. Ureteral obstruction is well known to occur at higher rates with transvaginal uterosacral ligament suspension than with other surgeries for pelvic organ prolapse, but this is often recognized at the time of cystoscopy and corrected iintraoperatively.
A review of 208 uterosacral ligament suspension procedures by Barbier et al found that ureteral compromise occurred in six of the 60 patients in whom a vaginal approach was used, but in none of the 148 patients in whom a laparoscopic approach was used. Although some of the cases of ureteral compromise in the vaginal group required only suture removal and replacement, a number required stent placement. [13]
Etiology
The 6 most common mechanisms of operative ureteral injury are as follows:
-
Crushing from misapplication of a clamp
-
Ligation with a suture
-
Angulation of the ureter with secondary obstruction
-
Transsection (partial or complete)
-
Resection of a segment of ureter
-
Ischemia from ureteral stripping or electrocoagulation
Any combination of these injuries may occur.
Factors that predispose a patient to iatrogenic urologic injury incllude the following:
-
Uterus size larger than 12 weeks' gestation
-
O varian cysts 4 cm or larger
-
Prior intra-abdominal surgery [11]
-
Radiation therapy
-
Advanced malignancy
-
Anatomical anomalies of the urinary tract
A systematic review of iatrogenic bladder and ureteric injuries sustained during cesarean delivery and hysterectomy concluded that surgeon inexperience was the prime risk factor for such injuries. However, the authors noted that the definition of inexperience varied among studies. [12]
Pathophysiology
The pathophysiology of ureteral injury depends on many factors, including the type of injury and when the injury is identified. Although spontaneous resolution and healing may occur, ureteral injuries may have numerous consequences, including the following:
-
Hydronephrosis with or without loss of kidney function
-
Urinary extravasation due to ureteral necrosis or unrecognized complete or partial transection
-
Ureteral stricture formation
Spontaneous resolution and healing
If the injury to the ureter is minor, easily reversible, and noticed immediately, the ureter may heal completely and without consequence. Inadvertent ligation of the ureter is an example of such an injury. If the ligation is noticed in a timely fashion, the suture can be cut off the ureter without significant injury.
Hydronephrosis
If complete ligation of the ureter occurs, the urine from the ipsilateral kidney is prevented from draining into the bladder, leading to hydronephrosis and progressive deterioration of ipsilateral kidney function. Acute obstruction will often present as renal colic, whereas chronic obstruction may be asymptomatic. If the urine in this obstructed system becomes infected, the patient will almost certainly become septic with pyonephrosis.
Urinary extravasation
Urinary extravation can occur if a patient has an unrecognized ligation of the ureter or a partial or complete ureteral transection. In complete unrecognized ligation of the ureter, a section of the ureteral wall necroses because of pressure-induced ischemia. The ischemic segment of the ureter eventually weakens, leading to urinary extravasation into the periureteral tissues and possible the adjacent peritoneum or retroperitoneum. Similarly, unrecognized partial or complete transection of the ureter resutls in extravasation of the urine. Urine leakage into the peritoneum results in urinary ascites, and if infected, peritonitis may ensue. Urine extravasation into the retroperitoneum or retropubic space may result in urinoma formation.
Ureteral stricture
Ureteral stricture may occur when the adventitial (outer) layer of the ureter is either stripped or electrocoagulated. The adventia of the ureter contains the ureteral blood supply (see the image below). When this is disturbed by stripping or electrocoagulation, ischemia to a particular segment of ureter may result. Ischemic strictures of the ureter may then develop, leading to obstruction and hydronephrosis of the ipsilateral kidney.
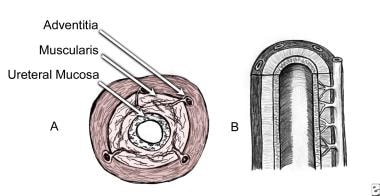 An illustration of the blood supply to the ureter running within the adventitial layer.
An illustration of the blood supply to the ureter running within the adventitial layer.
Uremia
Uremia results when ureteral injury causes total urinary obstruction. This may result from bilateral ureteral injury or from a unilateral injury occurring in a solitary functioning kidney. Anuria is the only immediate sign of imminent uremia. These cases require immediate intervention to preserve kidney function.
Presentation
Iatrogenic ureteral injury during gynecologic surgery may present either intraoperatively or postoperatively. Routine use of intraoperative cystoscopy increases the intraoperative detection rate of urinary tract injuries, but does not appear to have much effect on rates of postoperative injury detection. [6] Intraoperative consultation with a urologist must be obtained when the injury is recognized immediately; these patients are best treated with primary ureteral repair during the same operation.
More than 70% of the time, unilateral ureteral injury is noticed postoperatively. The patient may present with flank pain, prolonged ileus, fever, watery vaginal discharge, or mildly or significantly elevated serum creatinine levels. In cases of bilateral ureteral injury, anuria is the first clinical sign.
Indications
The indications for evaluation of ureteral injury following gynecologic procedures include the following:
-
Costovertebral angle tenderness
-
Unexplained fever
-
Persistent abdominal distention
-
Prolonged ileus
-
Unexplained hematuria
-
Escape of watery fluid through the vagina or abdominal incision
-
Appearance of a lower abdominal or pelvic mass
-
Oliguria or elevated serum creatinine levels from baseline (mild or significant)
Relevant Anatomy
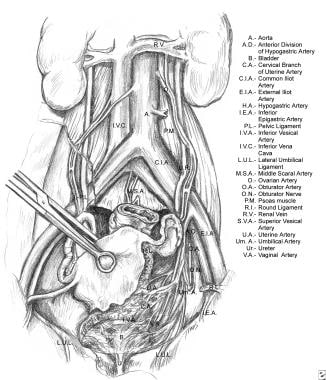
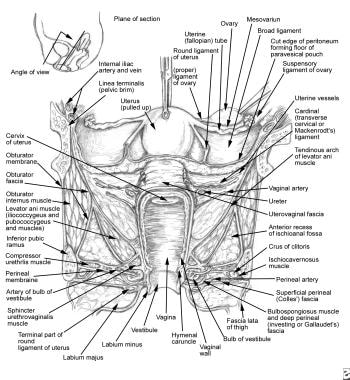
The relevant anatomy of the ureter is shown in the images below. Note the close proximity of the distal ureter to the uterine vessels. This is the site where injuries most commonly occur during gynecologic procedures. The next most commonly injured area is at the pelvic brim, in the area of the infundibulopelvic ligament.
 Relevant anatomy of the ureter, illustrating its course from the renal pelvis to the bladder. Note the ureter's proximity at the pelvic brim to the infundibulopelvic ligament.
Relevant anatomy of the ureter, illustrating its course from the renal pelvis to the bladder. Note the ureter's proximity at the pelvic brim to the infundibulopelvic ligament.
 Relevant anatomy of the ureter. Notice the proximity of the ureter to the uterine vessels at the level of the cervix. Most ureteral injuries following gynecologic surgery occur in this area.
Relevant anatomy of the ureter. Notice the proximity of the ureter to the uterine vessels at the level of the cervix. Most ureteral injuries following gynecologic surgery occur in this area.
-
An illustration of the blood supply to the ureter running within the adventitial layer.
-
Relevant anatomy of the ureter, illustrating its course from the renal pelvis to the bladder. Note the ureter's proximity at the pelvic brim to the infundibulopelvic ligament.
-
Relevant anatomy of the ureter. Notice the proximity of the ureter to the uterine vessels at the level of the cervix. Most ureteral injuries following gynecologic surgery occur in this area.
-
An illustration of the shape and configuration of a Boari flap.



