Practice Essentials
Bacterial abscess of the liver is relatively rare; however, it has been described since the time of Hippocrates (400 BCE), with the first published review by Bright appearing in 1936. In 1938, Ochsner's classic review heralded surgical drainage as the definitive therapy; however, despite the more aggressive approach to treatment, the mortality remained at 60-80%. [1]
The development of new radiologic techniques, the improvement in microbiologic identification, and the advancement of drainage techniques, as well as improved supportive care, have reduced mortality to 5-30%; yet, the prevalence of liver abscess has remained relatively unchanged. Untreated, this infection remains uniformly fatal.
The three major forms of liver abscess, classified by etiology, are as follows:
-
Pyogenic abscess, which is most often polymicrobial, accounts for 80% of hepatic abscess cases in the United States
-
Amebic abscess due to Entamoeba histolytica accounts for 10% of cases [2]
-
Fungal abscess, most often due to Candida species, accounts for fewer than 10% of cases
Treatment should include drainage, either percutaneous or surgical. Antimicrobial treatment is a common adjunct to percutaneous or surgical drainage. Antibiotic therapy as a sole treatment modality is not routinely advocated, though it has been successful in a few reported cases.
For patient education resources, see the Infections Center and the Digestive Disorders Center, as well as Skin Abscess and Antibiotics.
Pathophysiology
The liver receives blood from both systemic and portal circulations. Increased susceptibility to infections would be expected given the increased exposure to bacteria. However, Kupffer cells lining the hepatic sinusoids clear bacteria so efficiently that infection rarely occurs. Multiple processes have been associated with the development of hepatic abscesses (see the image below).
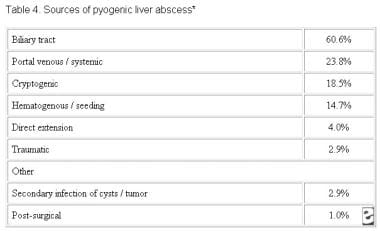 Table 4: Underlying etiology of 1086 cases of liver abscess compiled from the literature.
Table 4: Underlying etiology of 1086 cases of liver abscess compiled from the literature.
Appendicitis was traditionally the major cause of liver abscess. As diagnosis and treatment of this condition has advanced, its frequency as a cause for liver abscess has decreased to 10%.
Biliary tract disease is now the most common source of pyogenic liver abscess (PLA). Obstruction of bile flow allows for bacterial proliferation. Biliary stone disease, obstructive malignancy affecting the biliary tree, stricture, and congenital diseases are common inciting conditions. With a biliary source, abscesses usually are multiple, unless they are associated with surgical interventions or indwelling biliary stents. In these instances, solitary lesions can be seen.
Infections in organs in the portal bed can result in a localized septic thrombophlebitis, which can lead to liver abscess. Septic emboli are released into the portal circulation, trapped by the hepatic sinusoids, and become the nidus for microabscess formation. These microabscesses initially are multiple but usually coalesce into a solitary lesion.
Microabscess formation can also be due to hematogenous dissemination of organisms in association with systemic bacteremia, such as endocarditis and pyelonephritis. Cases also are reported in children with underlying defects in immunity, such as chronic granulomatous disease and leukemia.
Approximately 4% of liver abscesses result from fistula formation between local intra-abdominal infections.
Despite advances in diagnostic imaging, cryptogenic causes account for a significant proportion of cases; surgical exploration has impacted this minimally. These lesions usually are solitary in nature.
Penetrating hepatic trauma can inoculate organisms directly into the liver parenchyma, resulting in pyogenic liver abscess. Nonpenetrating trauma can also be the precursor to pyogenic liver abscess by causing localized hepatic necrosis, intrahepatic hemorrhage, and bile leakage. The resulting tissue environment permits bacterial growth, which may lead to pyogenic liver abscess. These lesions are typically solitary.
PLA has been reported as a secondary infection of amebic abscess, hydatid cystic cavities, and metastatic and primary hepatic tumors. It is also a known complication of liver transplantation, hepatic artery embolization in the treatment of hepatocellular carcinoma, and the ingestion of foreign bodies, which penetrate the liver parenchyma. Trauma and secondarily infected liver pathology account for a small percentage of liver abscess cases.
The right hepatic lobe is affected more often than the left hepatic lobe by a factor of 2:1. Bilateral involvement is seen in 5% of cases. The predilection for the right hepatic lobe can be attributed to anatomic considerations. The right hepatic lobe receives blood from both the superior mesenteric and portal veins, whereas the left hepatic lobe receives inferior mesenteric and splenic drainage. It also contains a denser network of biliary canaliculi and, overall, accounts for more hepatic mass. Studies have suggested that a streaming effect in the portal circulation is causative.
Etiology
Polymicrobial involvement is common, with Escherichia coli and Klebsiella pneumoniae being the two most frequently isolated pathogens (see the image below). Reports suggest that K pneumoniae is an increasingly prominent cause. [3]
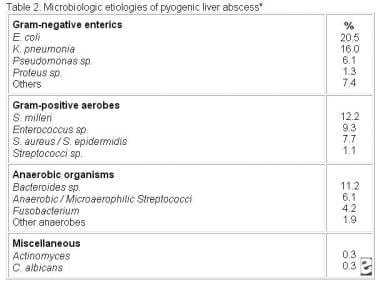 Table 2: Microbiologic results from 312 cases of liver abscess compiled from the literature.
Table 2: Microbiologic results from 312 cases of liver abscess compiled from the literature.
Enterobacteriaceae are especially prominent when the infection is of biliary origin. Abscesses involving K pneumoniae have been associated with multiple cases of endophthalmitis.
The pathogenic role of anaerobes was underappreciated until the isolation of anaerobes from 45% of cases of pyogenic liver abscess was reported in 1974. Since that time, increasing rates of anaerobic involvement have been reported, likely because of increased awareness and improved culturing techniques. The most frequently encountered anaerobes are Bacteroides species, Fusobacterium species, and microaerophilic and anaerobic streptococci. A colonic source is usually the initial source of infection.
Staphylococcus aureus abscesses usually result from hematogenous spread of organisms involved with distant infections, such as endocarditis. S milleri is neither anaerobic nor microaerophilic. It has been associated with both monomicrobial and polymicrobial abscesses in patients with Crohn disease, as well as with other patients with pyogenic liver abscess.
Amebic liver abscess is most often due to E histolytica. Liver abscess is the most common extraintestinal manifestation of this infection.
Fungal abscesses primarily are due to Candida albicans and occur in individuals with prolonged exposure to antimicrobials, hematologic malignancies, solid-organ transplants, and congenital and acquired immunodeficiency. Cases involving Aspergillus species have been reported.
Other organisms reported in the literature include Actinomyces species, Eikenella corrodens, Yersinia enterocolitica, Salmonella typhi, and Brucella melitensis.
A small case series in Taiwan investigated pyogenic liver abscess as the initial manifestation of underlying hepatocellular carcinoma. In regions with a high prevalence of both pyogenic liver abscess and hepatocellular carcinoma, clinicians should be aware of the possibility of underlying hepatocellular carcinoma in patients with risk factors for the disease. [4]
Epidemiology
United States statistics
The incidence of pyogenic liver abscess has essentially remained unchanged by both hospital and autopsy data. Liver abscess was diagnosed in 0.7%, 0.45%, and 0.57% of autopsies during the periods of 1896-1933, 1934-1958, and 1959-1968, respectively. The frequency in hospitalized patients is in the range of 8-16 cases per 100,000 persons. Studies suggest a small, but significant, increase in the frequency of liver abscess.
Age-related demographics
Prior to the antibiotic era, liver abscess was most common in the fourth and fifth decades of life, primarily due to complications of appendicitis. With the development of better diagnostic techniques, early antibiotic administration, and the improved survival of the general population, the demographic has shifted toward the sixth and seventh decades of life. Frequency curves display a small peak in the neonatal period followed by a gradual rise beginning at the sixth decade of life.
Cases of liver abscesses in infants have been associated with umbilical vein catheterization and sepsis.
When abscesses are seen in children and adolescents, underlying immune deficiency, severe malnutrition, or trauma frequently exists.
Sex-related demographics
While abscesses once showed a predilection for males in earlier decades, no sexual predilection currently exists. Males have a poorer prognosis from hepatic abscess than females.
Prognosis
Untreated, pyogenic liver abscess remains uniformly fatal. With timely administration of antibiotics and drainage procedures, mortality currently occurs in 5-30% of cases. The most common causes of death include sepsis, multiorgan failure, and hepatic failure. [5]
Indicators of a poor prognosis have been described since 1938 and include multiplicity of abscesses, underlying malignancy, severity of underlying medical conditions, presence of complications, and delay in diagnosis. [5]
Indicators of a poor prognosis in amebic abscess include a bilirubin level of greater than 3.5 mg/dL, encephalopathy, hypoalbuminemia (ie, serum albumin level of < 2 g/dL), and multiple abscesses; all are independent factors that predict poor outcome.
An underlying malignant etiology and an Acute Physiology and Chronic Health Evaluation (APACHE II) score greater than 9 increases the relative mortality by 6.3-fold and 6.8-fold, respectively.
Chen et al examined prognostic factors for elderly patients with pyogenic liver abscess. [6] Results from the study, which included 118 patients aged 65 years or older and 221 patients below age 65 years, indicated that age and an APACHE II score of 15 or greater at hospital admission were risk factors for mortality. The evidence ultimately suggested that outcomes for older patients with pyogenic liver abscess are on a par with those for younger patients. The investigators also found that in the younger patient group, there was greater frequency of males suffering from alcoholism, a cryptogenic abscess, and K pneumoniae infection.
-
Table 1: Presenting symptoms and signs in 715 patients diagnosed with liver abscess.
-
Table 2: Microbiologic results from 312 cases of liver abscess compiled from the literature.
-
Table 3: Comparison of the radiologic procedures used in the diagnosis of liver abscess.
-
Table 4: Underlying etiology of 1086 cases of liver abscess compiled from the literature.
-
Computed tomography (CT) scan findings of liver abscess are shown. A large, septated abscess of the right hepatic lobe is revealed. Abscess was successfully treated with percutaneous drainage and antimicrobial therapy.
-
Computed tomography (CT) scan findings of liver abscess are shown. A large anterior abscess involving the left hepatic lobe is revealed. Abscess was successfully treated with percutaneous drainage and antimicrobial therapy.




