Practice Essentials
Glioblastoma (GBM), formerly known as glioblastoma multiforme, is the most common and malignant of adult gliomas. [1] Gliomas are primary neoplasms of the central nervous system that arise from glial cells or their progenitors. See the image below.
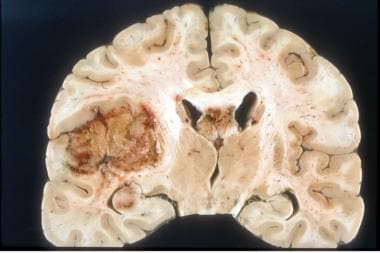 Coronal section of a glioblastoma in the left temporal lobe with typical coloration: thickened tan cortex overlying a large central region of yellowish necrosis stippled with red and brown lesions from new and old hemorrhage. Courtesy of Wikimedia Commons [author Sbrandner, https://commons.wikimedia.org/wiki/File:Glioblastoma_macro.jpg].
Coronal section of a glioblastoma in the left temporal lobe with typical coloration: thickened tan cortex overlying a large central region of yellowish necrosis stippled with red and brown lesions from new and old hemorrhage. Courtesy of Wikimedia Commons [author Sbrandner, https://commons.wikimedia.org/wiki/File:Glioblastoma_macro.jpg].
In the fifth edition of the World Health Organization (WHO) Classification of Central Nervous System (CNS) Tumors, published in 2021, [2] glioblastoma was redefined according to molecular testing with respect to isocitrate dehydrogenase (IDH) status. Previously, glioblastoma had included high-grade IDH-wildtype and IDH-mutant neoplasms. The term glioblastoma is now exclusively used to describe adult IDH-wildtype tumors. Highest-grade IDH-mutant tumors have been reclassified as astrocytoma IDH-mutant CNS WHO grade 4. The term glioblastoma multiforme is no longer used, and the term glioblastoma is no longer applied to pediatric tumors. [3]
The 2021 WHO classification defines glioblastoma as an adult grade 4 diffuse astrocytic glioma that is IDH-wildtype and H3-wildtype and has one or more of the following histologic or genetic features [3, 2] :
-
Microvascular proliferation
-
Necrosis
-
TERT promoter mutation
-
EGFR gene amplification
-
+7/-10 chromosome copy number change
For more information on the new diagnostic criteria, see Background.
Throughout this article, glioblastoma will refer exclusively to glioblastoma IDH-wildtype CNS WHO grade 4 unless stated otherwise. Astrocytoma IDH-mutant CNS WHO grade 4 is discussed in Astrocytoma.
Glioblastoma has three distinct histologic variants: giant cell glioblastoma, gliosarcoma, and epithelioid glioblastoma (see Workup/Histologic Findings). [3]
Signs and symptoms
The clinical history of a patient with GBM is usually short (< 3 months in > 50% of patients). [4] The most common presenting signs and symptoms are seizure and cognitive disorder. [5] Other presenting symptoms include the following [6] :
-
Slowly progressive focal neurologic deficits—eg, motor weakness, sensory loss, memory loss, language deficits, visual impairments.
-
Generalized manifestations of increased intracranial pressure—eg, headaches, nausea and vomiting, personality changes, cognitive impairment
The etiology of GBM is unknown in most cases. Suggested causes include the following:
-
Head injury, N-nitroso compounds, occupational hazards, electromagnetic field exposure (all inconclusive) [16]
See Presentation for more detail.
Diagnosis
Because GBM is now a molecular diagnosis, genetic studies for IDH and H3 status are essential, and genetic studies for TERT promoter mutation, EGFR gene amplification, and +7/-10 chromosome copy number changes are important as well. Tumor genetics are also useful for predicting response to adjuvant therapy.
Imaging studies of the brain are essential for diagnosis. Magnetic resonance imaging (MRI), with and without contrast, is the study of choice. [19, 20] Other possible studies include the following [21] :
-
Computed tomography (CT)
-
Positron emission tomography (PET)
-
Magnetic resonance spectroscopy (MRS)
Cerebral angiography is not necessary
Other diagnostic measures that may be considered include the following:
-
Electroencephalography (EEG): May show suggestive findings, but findings specific for GBM will not be observed
-
Lumbar puncture (LP): Occasionally used for differential diagnosis but not necessary; cerebrospinal fluid studies do not significantly facilitate diagnosis of GBM
Staging is not practiced. These tumors do not have clearly defined margins; they tend to invade locally and spread along white matter pathways, creating the appearance of multiple GBMs or multicentric gliomas on imaging studies. GBM is not known to metastasize outside of the central nervous system.
See Workup for more detail.
Management
No current treatment is curative. Standard treatment consists of biopsy or resection followed by early (< 48 h) postoperative MRI or CT and medical care. [22] Choice of therapy is based on patient age, performance status, and MGMT methylation status, as follows:
-
Patients ≤70 years with good performance status (Karnofsky Performance Scale score [KPS] ≥60), regardless of MGMT methylation status: Fractionated standard brain radiation therapy (RT) plus concurrent and adjuvant temozolomide (TMZ), with or without alternating electric field therapy
-
Patients ≤70 years with poor performance status (KPS < 60), regardless of MGMT methylation status: Hypofractionated brain RT with or without concurrent or adjuvant TMZ, or TMZ alone, or palliative care alone
-
Patients > 70 years with good performance status (KPS ≥60) and MGMT promoter-methylated tumors: Hypofractionated brain RT plus concurrent and adjuvant TMZ or standard brain RT plus concurrent and adjuvant TMZ and alternating electric field therapy
-
Patients > 70 years with good performance status (KPS ≥60) and MGMT unmethylated or indeterminant tumors: Standard brain RT plus concurrent and adjuvant TMZ and alternating electric field therapy.
-
Patients > 70 years with poor performance status (KPS < 60), regardless of MGMT methylation status: Hypofractionated brain RT alone, or TMZ alone, or palliative care alone.
-
Supportive care for clinical manifestations (eg, headache, seizures, venous thromboembolism)
Surgical options include biopsy, subtotal resection, and gross total resection (associated with better survival). Because GBM cannot be cured surgically, the surgical goals are as follows [23] :
-
Establish a pathologic diagnosis
-
Relieve any mass effect
-
If possible, achieve a gross total resection to facilitate adjuvant therapy
-
Minimize postoperative neurologic deficit
In some cases, stereotactic biopsy is followed by RT (eg, for patients with a tumor located in an eloquent area of the brain, patients whose tumors have minimal mass effect, and patients in poor medical condition who cannot undergo general anesthesia). In several studies, the extent of surgery has been shown to affect length of survival. [24, 25, 26, 27, 28, 29, 30]
Key points regarding RT for GBM include the following:
-
The responsiveness of GBM to radiotherapy varies. [35]
-
Interstitial brachytherapy, in which radioactive seeds are placed intraoperatively, after tumor resection, allows immediate initiation of RT. [36]
-
RT and/or radiosurgery for recurrent GBM is controversial but recommended under certain conditions. [41]
The optimal chemotherapeutic regimen for GBM is not yet defined, but adjuvant chemotherapy appears to yield a significant survival benefit in some patients. [42, 43, 44, 45, 31, 46, 34] Agents used include the following:
-
Temozolomide
-
Nitrosoureas (eg, lomustine, carmustine)
-
Bevacizumab (alone or with irinotecan) for recurrent cases
-
Tyrosine kinase inhibitors (eg, regorafenib, gefitinib, erlotinib)
-
Investigational therapies
Because GBM cannot be cured, regular follow-up to monitor for progression/recurrence is essential and consists of brain MRI 2-8 weeks after RT, then every 2-4 months for 3 years, then every 3-6 months indefinitely. [23]
See Treatment and Medication for more detail.
For patient education resources, see the Brain Cancer Resource Center as well as the patient education article Brain Cancer from the American Brain Tumor Association (ABTA).
Background
Of the estimated 83,750 primary brain and other central nervous system tumors diagnosed in the United States in 2021, approximately 20,800 (or 24.84%) were gliomas. [47] Gliomas arise from glial cells (ie, astrocytes, oligodendrocytes, ependymal cells) or their precursors and comprise a heterogeneous group of neoplasms that differ in location within the central nervous system, age and sex distribution, growth potential, extent of invasiveness, morphologic features, tendency for progression, and treatment response. [48] Glioblastoma (GBM), formerly known as glioblastoma multiforme, is by far the most common and most malignant of the glial tumors, accounting for approximately 45-55% of all gliomas and 12-15% of all primary brain tumors. [48, 49, 50, 47]
Previously, in the 2016 revision of the fourth edition of the World Health Organization (WHO) Classification of Central Nervous System (CNS) Tumors, glioblastomas were divided into three classes according to isocitrate dehydrogenase (IDH) mutation status: IDH wildtype; IDH mutant; and not otherwise specified (NOS), which was applied to tumors for which IDH evaluation could not be performed. [51, 52]
IDH-wildtype GBMs corresponded closely to the clinically defined “primary” glioblastomas, a historical term describing GBMs that manifested de novo (ie, without evidence of a pre-existing, less-malignant precursor lesion), typically affected older patients, and were associated with a short clinical history and poor prognosis. [4, 53, 54, 52] IDH-mutant GBMs corresponded closely to “secondary” glioblastomas—GBMs that developed through malignant progression from a low-grade astrocytoma (WHO grade II) or anaplastic astrocytoma (WHO grade III), typically affected younger patients, and were associated with a longer clinical history and better prognosis. [4, 53, 54, 52]
In 2021, the fifth edition of the WHO Classification of CNS Tumors updated the diagnostic criteria for glioblastoma to reflect increasing evidence that IDH-wildtype and IDH-mutant glioblastomas constitute distinct disease entities that evolve through different genetic pathways, affect different patient populations, and respond to different therapies. [3, 2] The term “IDH-mutant glioblastoma” was eliminated, and all tumors previously classified as IDH-mutant glioblastoma were reclassified as astrocytoma IDH-mutant CNS WHO grade 4.
To be considered a glioblastoma under the new guidelines, a tumor must be a diffuse astrocytic glioma, must be IDH-wildtype, must affect an adult (the term “glioblastoma” is no longer applied to pediatric tumors), and must possess any one of the following histopathological or molecular features: microvascular proliferation, necrosis, TERT promoter mutation, EGFR gene amplification, or +7/−10 chromosome copy number changes. [2] In keeping with the 2021 classification, throughout this article, the term glioblastoma will refer exclusively to glioblastoma IDH-wildtype CNS WHO grade 4 unless stated otherwise. Astrocytoma IDH-mutant CNS WHO grade 4 is discussed in Astrocytoma.
The fifth edition of the WHO Classification of CNS Tumors recognizes three distinct histologic variants of glioblastoma: giant cell glioblastoma, gliosarcoma, and epithelioid glioblastoma. [2] For more information on the differences between these variants, see Workup/Histologic Findings.
Composed of a heterogeneous mixture of poorly differentiated neoplastic astrocytes, glioblastomas occur most often in the subcortical white matter and deeper grey matter of the cerebral hemispheres. [55, 56, 57] In many cases, tumor infiltration extends into the adjacent cortex or the basal ganglia. When a tumor in the frontal cortex spreads across the corpus callosum into the contralateral hemisphere, it creates the appearance of a bilateral symmetric lesion, hence the term “butterfly glioma” (see the image below) Far less frequently, glioblastoma affects the brainstem, the cerebellum, or the spinal cord; if a tumor is identified in these midline locations, other forms of diffuse glioma should be considered (eg, diffuse midline glioma, H3 K27 altered). [2]
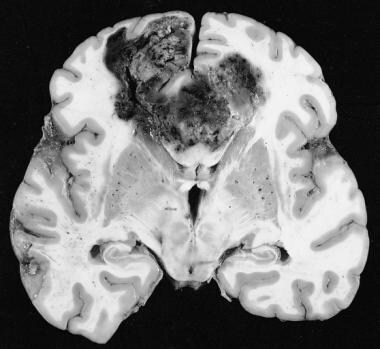 This typical untreated glioblastoma, here with the classic "butterfly" configuration, is a necrotic hemorrhagic mass. Courtesy of Wikimedia Commons [author Rodney D McComb, MD and The Armed Forces Institute of Pathology, https://commons.wikimedia.org/wiki/File:Glioblastoma_multiforme.jpg].
This typical untreated glioblastoma, here with the classic "butterfly" configuration, is a necrotic hemorrhagic mass. Courtesy of Wikimedia Commons [author Rodney D McComb, MD and The Armed Forces Institute of Pathology, https://commons.wikimedia.org/wiki/File:Glioblastoma_multiforme.jpg].
In contrast to astrocytomas IDH-mutant CNS WHO grade 4, which develop from lower-grade astrocytomas (WHO grade 2 or 3) glioblastomas IDH-wildtype CNS WHO grade 4 manifest de novo, without any evidence of a pre-existing, less-malignant precursor lesion. Patients typically present after a short clinical history (usually less than 3 months). [4] Treatment is palliative and includes surgery, radiotherapy, and chemotherapy. [58, 23, 59]
Pathophysiology
Origin
Single-cell RNA sequencing of human tumors has shown that glioblastomas (as previously defined, including pediatric glioblastomas) are composed of a heterogeneous mixture of poorly differentiated neoplastic cells that recapitulate various neurodevelopmental trajectories (eg, astrocyte-like, neural progenitor–like, and oligodendrocytic progenitor–like) and are affected by interactions with immune cells (mesenchymal-like). [60] While mouse models of glioblastoma have shown that a variety of central nervous system cell types—including astrocytes, neurons, oligodendrocyte precursors, and neural precursors—can transform into malignant cells that recapitulate features of glioblastoma, [61, 62] multiple lines of inquiry suggest that the most likely cell of origin is a neural precursor in the subventricular zone. [63, 64, 65]
Location
Glioblastomas are preferentially located in the subcortical white matter and deeper grey matter of the cerebral hemispheres and affect all cerebral lobes. [55, 56, 57] Reports of the most commonly affected lobes vary, with one study finding that glioblastoma most frequently affects the temporal lobe (followed by the insula, parietal lobes, and near the periventricular area frontally and occipitally), [56] and another showing that glioblastoma most frequently affects the frontal lobe (followed by temporal, parietal, and occipital). [57] Other sites for glioblastoma that are much less common include the brainstem, the cerebellum, and the spinal cord. [66] With lesions in those locations, other forms of diffuse glioma should be considered (eg, diffuse midline glioma, H3 K27 altered).
Invasion
Glioblastomas often spread along white matter tracts (eg, the corpus callosum, internal capsule, optic radiation, anterior commissure, fornix, and subependymal regions), but infiltration can also involve cortical and deep gray matter structures (eg, the basal ganglia). [2] When a tumor in the frontal cortex spreads across the corpus callosum into the contralateral hemisphere, it creates the appearance of a bilateral symmetric lesion, hence the term “butterfly glioma” (see the image below).
This typical untreated glioblastoma, here with the classic "butterfly" configuration, is a necrotic hemorrhagic mass. Courtesy of Wikimedia Commons [author Rodney D McComb, MD and The Armed Forces Institute of Pathology, https://commons.wikimedia.org/wiki/File:Glioblastoma_multiforme.jpg].
A subset of glioblastomas (0.5-35% in different studies) manifest as multiple lesions and are referred to as either “multifocal” or “multicentric.” [67, 68, 69, 70] Multifocal glioblastomas spread contiguously between multiple foci, while multicentric glioblastomas are distinct, widely separated lesions. Multifocal glioblastomas appear to be more common than multicentric glioblastoma, as careful histologic analyses have shown that only 2.4% of glioblastomas are truly multiple independent tumors. [71, 72] The genetic and pathologic mechanisms driving multifocality are unclear, but studies have shown that these tumors typically have EGFR gene amplifications as well as TERT promotor and PTEN mutations. [73]
In contrast to low-grade CNS malignancies, glioblastomas contain extensive hypoxic areas—ie, regions where oxygen demand exceeds oxygen supply. [2] These hypoxic areas occur in GBM due to rapid cell proliferation and erratic neovascularization that leads to poor oxygen diffusion. [74] Hypoxia increases tumor aggressiveness, promoting the migration of glioblastoma cells and infiltration of surrounding healthy brain tissue, which in turn makes curative surgical resection impossible. [75]
Although glioblastomas can seed the cerebrospinal fluid via drop metastases or growth along ventricular surfaces, invasion of the dura mater, venous sinuses, and bone is rare. [76, 77, 78, 79, 80, 81] Extracranial metastases are also uncommon, occurring in just 0.4-0.5% of cases. [82, 83] The infrequency of metastasis has been attributed to immune mechanisms that disrupt implantation and growth in conjunction with the short survival of glioblastoma patients. [2, 84, 85, 82, 83] When metastases do occur, they usually manifest at the time of recurrence and infiltrate bones, lymph nodes, liver, and lungs. [82, 83] Historical case studies have also implicated ventricular shunts as a vehicle for rare extraneural metastases. [86, 87]
Microvascular Proliferation
One of the histopathologic hallmarks of glioblastoma is microvascular proliferation—the rapid growth of small-lumen, multilayered blood vessels. [2] (See the image below.) Characterized by the formation of two or more blood vessels that share a common wall of endothelial and smooth muscle cells, microvascular proliferation typically occurs in the hypoxic core of glioblastomas, where new capillaries sprout from pre-existing vessels. [88]
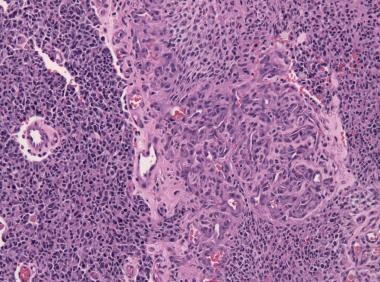 Hematoxylin and eosin stain of a biopsy specimen of a glioblastoma shows prominent microvascular proliferation (formation of a mulitlayered "glomeruloid tuft"). Courtesy of Wikimedia Commons [author Jensflorian, https://commons.wikimedia.org/wiki/File:Glioblastoma_endothelial_proliferations.jpg].
Hematoxylin and eosin stain of a biopsy specimen of a glioblastoma shows prominent microvascular proliferation (formation of a mulitlayered "glomeruloid tuft"). Courtesy of Wikimedia Commons [author Jensflorian, https://commons.wikimedia.org/wiki/File:Glioblastoma_endothelial_proliferations.jpg].
Microvascular proliferation is driven by several mechanisms, including hypoxia-induced endothelial proliferation, secretion of angiogenic factors (eg, vascular endothelial growth factor [VEGF]) by tumor cells, and incorporation of tumor cells into vascular endothelium. [88] The final result of microvascular proliferation is the formation of large-lumen microvessels that often have a glomeruloid shape and visible mitoses. [89, 90] Although interactions between blood vessels and tumor cells during microvascular proliferation are known to promote tumor growth, [91, 92] studies exploring the use of the anti-VEGF monoclonal antibody bevacizumab in the treatment of glioblastoma have produced conflicting results. [93, 94]
Necrosis
The other defining histopathologic feature of glioblastoma is necrosis, or cell death (see the image below). Several mechanisms have been proposed to explain the occurrence of necrosis in GBM. One hypothesis is that the vessels formed during microvascular proliferation have poorly formed, thrombogenic luminal surfaces. This thrombogenicity is exacerbated by the secretion of pro-coagulation molecules (eg, tissue factor) from glioblastoma cells. [95] As microthrombi form, the surrounding tissue becomes infarcted, leading to necrosis and creating an acidic, hypoxic, and hypoglycemic microenvironment. Nearby glioblastoma cells retreat from this hostile microenvironment, forming the characteristic pseudopalisades of less-proliferative, hypoxia-inducible factor 1-alpha (HIF1-α)–secreting cells. [96, 97]
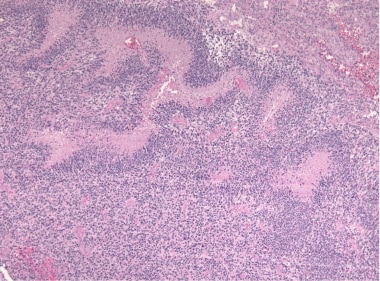 Necrosis is another histopathologic hallmark of glioblastoma. As seen here, necrotic areas often create serpentine patterns, and tumor cells form pseudopalisades around the periphery of these necrotic areas. Courtesy of Wikimedia Commons [author Jensflorian, https://commons.wikimedia.org/wiki/File:GBM_pseudopalisading_necrosis.jpg].
Necrosis is another histopathologic hallmark of glioblastoma. As seen here, necrotic areas often create serpentine patterns, and tumor cells form pseudopalisades around the periphery of these necrotic areas. Courtesy of Wikimedia Commons [author Jensflorian, https://commons.wikimedia.org/wiki/File:GBM_pseudopalisading_necrosis.jpg].
Mutations
Of all the astrocytic neoplasms, glioblastomas contain the greatest number of genetic changes. In most cases these result from the accumulation of multiple mutations. Some of the more common genetic abnormalities, including the three diagnostic mutations, are described below.
Epidermal growth factor receptor (EGFR)
The EGFR gene encodes a transmembrane receptor tyrosine kinase involved in the regulation of cell proliferation. [98] Approximately 60% of glioblastomas show evidence of EGFR alterations. [98] While multiple alterations have been identified—including amplification, mutation, fusion, rearrangement, and altered splicing—all clinically relevant changes increase activity of the EGFR gene and, ultimately, promote proliferation, invasion, and resistance to radiotherapy and chemotherapy. [99, 100] The most frequent alteration is EGFR amplification, which occurs in roughly 40% of glioblastomas. [101, 102]
Several trials exploring EGFR-targeted therapy have failed to produce meaningful results, likely due to a combination of the heterogeneity of EGFR alterations in GBM, low drug specificity, and poor brain penetration. [103] However, recent studies have shown that EGFR has pro-survival kinase-independent functions in glioblastoma cells, which has inspired novel approaches to EGFR-targeted therapy.[ [104, 105]
Telomerase reverse transcriptase (TERT) promoter
The TERT gene encodes a reverse transcriptase subunit of telomerase, a ribonucleoprotein responsible for repairing telomeres damaged during cellular replication, thereby maintaining telomere length and preventing cell death. [106] Telomere lengthening is required for the infinite proliferation of tumor cells, and thus TERT promoter mutations, which are associated with increased telomerase activity, contribute to tumorigenesis in glioblastoma. [107]
Two TERT promoter mutations—C228T and C250T—result in the upregulation of TERT expression and have been reported in nearly 80% of glioblastomas. [106, 108] While some studies have reported a negative association between TERT promoter mutations and survival in glioblastoma patients, [109, 110] others have failed to report this, [111, 112] and the prognostic significance of TERT remains uncertain. [113] While various telomerase-inhibiting therapies are being explored in preclinical and clinical trials, [114, 115, 116] none has yet been approved for clinical care in glioblastoma.
+7/−10 chromosome copy number changes
Whole chromosome gain (trisomy 7) and whole chromosome 10 loss (monosomy 10) are among the most common numerical chromosome alterations in glioblastoma. [117] They frequently occur in combination (+7/-10); less frequent are isolated gains in chromosome 7 or isolated losses in chromosome 10. The sensitivity and specificity of +7/-10 for glioblastoma are 59% and 98%, respectively. [102] Copy number variations in chromosomes 7 and 10 are some of the earliest events in glioblastoma tumor development. [118] The EGFR gene is located on the short arm of chromosome 7 (7p11. 2), and thus, gain of chromosome 7 is associated with EGFR amplification. [118] These mutations are associated with a poor prognosis. [2]
The p14ARF-MDM2-MDM4-p53 pathway
The p53 pathway is an essential component of DNA repair, cell cycle arrest, and apoptosis. Alterations in this pathway are extremely common, occurring in nearly 90% of glioblastomas. [118, 119] Mutations in p53, the classic tumor suppressor gene, are present in 20-25% of glioblastomas. [118, 120] Mutations in MDM4 and MDM2, upstream inhibitors of p53, constitute an alternative mechanism by which tumor cells can escape p53-regulated control of cellular proliferation and occur in roughly 15% of glioblastomas. [118] Furthermore, MDM2 is inhibited by p14ARF, an alternate reading frame protein encoded by the COKN2A locus, which is deleted in approximately 60% of glioblastomas. [118, 119] Curiously, mutations in p14ARF, MDM2, MDM4, and p53 usually occur in isolation from one another. [118]
PTEN and the PI3K-AKT-mTOR pathway
The PI3K pathway, an important regulator of cellular proliferation, is activated by RAS and/or receptor tyrosine kinases (including EGFR—see above) and inhibited by the tumor suppressor gene PTEN, which is located on the long arm of chromosome 10 (10q23.3) and encodes a tyrosine phosphatase. Alterations in this pathway are present in roughly 90% of glioblastomas, and amplifications involving EGFR are especially common. [118, 119] Mutations in or deletion of PTEN are less frequent, occurring in approximately 40% of glioblastomas. [121, 118] PTEN mutations increase resistance to multiple therapies and are strongly associated with shorter survival in glioblastoma patients. [122, 123]
Other mutations
Less frequent but more malignant mutations in glioblastomas include the following:
-
MMAC1-E1: This gene is involved in the progression of gliomas to their most malignant form.
-
MAGE-E1: This glioma-specific member of the MAGE family is expressed at up to 15-fold higher levels in glioblastoma than in normal astrocytes.
-
NRP/B: This gene codes for nuclear-restricted protein/brain, which is expressed in neurons but not in astrocytes ( NRP/B mutants are found in glioblastoma cells.)
Additional genetic alterations in primary glioblastomas include p16 deletions (30-40%), p16INK4A, and retinoblastoma (RB) gene protein alterations. [118, 119]
Etiology
The etiology of glioblastoma remains unknown in most cases. Familial gliomas account for approximately 5% of malignant gliomas, and less than 1% of gliomas are associated with a known genetic syndrome (e.g., neurofibromatosis type 1, Turcot syndrome, Lynch syndrome, Li-Fraumeni syndrome). [7, 8]
The only established non-genetic risk factor for glioblastoma is ionizing radiation to the head or neck. [8, 124] Ionizing radiation is the type of radiation produced by atomic bombs, therapeutic radiation, CT scans, MRI scans, and x-rays. However, while survivors of atomic bomb radiation and patients who receive therapeutic radiation for lymphoblastic leukemia are more likely to develop glioblastoma, [125, 126] patients who receive diagnostic irradiation (ie, CT, MRI, x-ray) do not appear to be at increased risk. [127] Regarding the former, higher doses of radiation are associated with a greater risk of developing glioblastoma and a shorter latency period. [9, 10]
Although concerns have been raised regarding cell phone use as a potential risk factor for development of gliomas, study results have been inconsistent, and this possibility remains controversial. The largest studies have not supported cell phone use as a cancer risk factor. [11, 12, 13, 14, 15, 17, 18]
Studies of association with head injury, N-nitroso compounds, occupational hazards, and electromagnetic field exposure have been inconclusive. [16]
There is a growing consensus that atopic conditions, including asthma, hay fever, eczema, and food allergies, are protective, reducing the risk of various forms of glioma—including glioblastoma—by nearly 40%. [9, 128, 129] This relationship is thought to be due to increased immune surveillance in patience with allergies, but more research is required to elucidate the underlying mechanisms.
Epidemiology
Glioblastoma is the most frequent malignant brain tumor in adults, accounting for approximately 12-15% of all primary intracranial neoplasms and 45-55% of all gliomas. [49, 50, 47] The overall incidence of glioblastoma varies worldwide and is highest in North America, Australia, and Northern and Western Europe. [130, 131] In the United States, the average annual age-adjusted incidence rate of GBM is 3.19 per 100,000 persons, and the overall prevalence is 9.23 per 100,000 persons. [49] Recent studies have shown that incidence is increasing in England, [132] but there does not appear to be any trend toward increased incidence in the United States or Canada. [133] These discrepancies may be due to differences in genetics or environmental factors, but they are more likely a reflection of international differences in surveillance procedures, reporting practices, and changes in classifications of glioblastoma over time. [51]
In the United States, glioblastoma is 1.59 times more common in males than females, with an annual age-adjusted incidence of 4.03 and 2.54 per 100,000 persons, respectively. [134] With regard to race and ethnicity, incidence is highest among non-Hispanic whites (3.51 per 100,000 persons) and lowest among Asians or Pacific Islanders (1.18 per 100,000 persons). [134]
Glioblastoma may manifest in persons of any age but preferentially affects older adults. The incidence rate increases with age, peaking at 75-79 years, and the median age at diagnosis is 64 years. [49, 135]
Although existing epidemiologic data are based on the previous WHO guidelines, implementation of the 2021 WHO guidelines is unlikely to result in a substantial change in incidence rates, because approximately 90% of all GBMs were IDH-wildtype while just 10% were IDH-mutant. [51, 136] However, because IDH-mutant GBM were more common in young people and in women, there will likely be a notable increase in the average age of onset and the incidence for men. [136]
Prognosis
Glioblastomas are among the most malignant of human neoplasms and have one of the worst survival rates of any brain tumor [49] —without therapy, glioblastoma patients have a median survival of 3 months. [137] Although current treatments remain palliative, they do prolong survival, and patients treated with optimal therapy—including surgical resection, radiation therapy, and chemotherapy—have a median survival of approximately 15-18 months. [138, 139]
There has been a significant increase in both 1-year and 5-year survival rates over the past 25 years. From 1997 to 2012, 1-year survival increased from 24.3% to 43.0%, and 5-year survival increased from 2.1% to 5.6%. [139, 140] These trends are likely due to widespread adoption of the current standard therapy in the early-mid 2000s as well as increased screening and earlier detection due to improvements in imaging technology. [141] It is important to note, however, that these data apply to GBM as previously defined by the WHO (ie, as an IDH-wildtype or IDH-mutant grade IV astrocytoma) and that the prognosis for GBM as currently defined has yet to be determined.
Patient survival depends on a variety of clinical parameters. Younger age, higher Karnofsky Performance Scale (KPS) score at presentation (the KPS is a standard measure of the ability of cancer patients to perform daily tasks), radiotherapy, and chemotherapy all correlate with improved outcome. [142, 143, 141] Clinical evidence also suggests that a greater extent of resection favors longer survival, [144, 145, 146] and tumors deemed unresectable due to location (eg, in the brainstem) portend a poorer prognosis. [147] Despite identification of multiple factors that influence survival, individual prediction of clinical outcome has remained an elusive goal.
The elderly (ie, persons 65 years of age or older) represent an important subgroup among glioblastoma patients, as they are more likely than their younger counterparts to suffer from medical comorbidities and polypharmacy, delays in diagnosis (early symptoms of GBM may be misinterpreted as signs of dementia or depression), treatment toxicities, precarious living situations with few social supports, and reduced functional and cognitive reserve (corresponding to a lower KPS score). [148, 149] These factors collectively translate to a significantly worse prognosis: among patients over 65, the 5-year survival rate is just 2.1% compared to 4.1% for those 55 to 64 and 6.5% for those 45 to 54. [150]
Because the elderly are underrepresented in clinical trials, there are few data to guide clinical decision-making for this population. However, two reviews of outcomes in elderly patients have been published. One found that gross-total resection confers a modest survival benefit and that treatment with bevacizumab significantly increases overall survival. [93] The second study confirmed that there is a survival advantage for patients who undergo maximal safe resection. It also found that radiotherapy extends survival in selected patients and that temozolomide chemotherapy is safe and extends the survival of patients with tumors that harbor MGMT promoter methylation. [151]
Recurrence, or regrowth of tumor after a period of complete remission or stable disease, is nearly universal in glioblastoma and typically occurs within 7 months of initial treatment. [45, 152] Prognosis at recurrence is grim, with an estimated median survival of 22-44 weeks. [45, 31] {ref 308} [153, 154] A review by Perrini et al of 48 patients with recurrent glioblastoma found that preoperative performance status at recurrence and subtotal versus gross-total repeat resection were independent predictors of survival. [155] These authors concluded that gross-total resection at repeat craniotomy is associated with longer overall survival and should be performed whenever possible in patients with recurrent glioblastoma who have good performance status. [155]
While the past few decades have seen marginal improvements in overall survival, new approaches to the management of glioblastoma are clearly needed. Novel approaches, such as the use of gene therapy and immunotherapy, as well as improved methods for the delivery of antiproliferative, antiangiogenic, and noninvasive therapies provide hope for the future, and continued enrollment of patients in clinical trials will generate important information on the efficacy of these investigational therapies. More information on these developments can be found under Investigational Approaches.
Patient Education
For patient education information, see the Brain Cancer Resource Center. In addition, information about glioblastoma (and other brain tumors) is available from the American Brain Tumor Association (ABTA) at About Brain Tumors.
-
Axial CT scan without intravenous contrast reveals a large right temporal intra-axial mass (glioblastoma). Extensive surrounding edema is present, as demonstrated by the peritumoral hypodensity, and a moderate right-to-left midline shift can be noted. All of the radiologic studies in this article are of the same patient.
-
A T1-weighted axial MRI without intravenous contrast demonstrates a hemorrhagic multicentric glioblastoma in the right temporal lobe. Effacement of the ventricular system is present on the right, along with mild impingement of the right medial temporal lobe on the midbrain.
-
A T1-weighted axial MRI with intravenous contrast shows heterogeneous enhancement of the lesion within the right temporal lobe. The hypointensity circumscribed within the enhancement is suggestive of necrosis. This radiologic appearance is typical of a multicentric glioblastoma.
-
A T1-weighted coronal MRI with intravenous contrast demonstrates a glioblastoma within the medial temporal lobe and the stereotypical pattern of contrast enhancement.
-
A T1-weighted sagittal MRI with intravenous contrast demonstrates a glioblastoma.
-
On T2-weighted axial MRI, the tumor (glioblastoma) and surrounding white matter within the right temporal lobe show increased signal intensity compared with a healthy brain, suggesting extensive tumorigenic edema.
-
A fluid-attenuated inversion recovery (FLAIR) axial MRI. This image is similar to the T2-weighted image and demonstrates extensive edema in a patient with glioblastoma.
-
Histopathologic slide demonstrating classic glioblastoma (GBM).
-
Magnetic resonance (MR) spectroscopy signal representative of glioblastoma (GBM) demonstrating a high peak ratio of choline (CHO) to creatine (CR), a decreased N-acetylaspartate (NAA) peak, and an increased lactate (LAC) peak.
-
Hematoxylin and eosin stain of a biopsy specimen of a glioblastoma shows prominent microvascular proliferation (formation of a mulitlayered "glomeruloid tuft"). Courtesy of Wikimedia Commons [author Jensflorian, https://commons.wikimedia.org/wiki/File:Glioblastoma_endothelial_proliferations.jpg].
-
Necrosis is another histopathologic hallmark of glioblastoma. As seen here, necrotic areas often create serpentine patterns, and tumor cells form pseudopalisades around the periphery of these necrotic areas. Courtesy of Wikimedia Commons [author Jensflorian, https://commons.wikimedia.org/wiki/File:GBM_pseudopalisading_necrosis.jpg].
-
Coronal section of a glioblastoma in the left temporal lobe with typical coloration: thickened tan cortex overlying a large central region of yellowish necrosis stippled with red and brown lesions from new and old hemorrhage. Courtesy of Wikimedia Commons [author Sbrandner, https://commons.wikimedia.org/wiki/File:Glioblastoma_macro.jpg].
-
Histology section of a giant cell glioblastoma. Several bizarre, multinucleated giant cells are visible against a background of smaller tumor cells. Courtesy of Wikimedia Commons (author Jensflorian, https://commons.wikimedia.org/wiki/File:Giant_cell_glioblastoma_HE_X200.jpg].
-
Histology section of a gliosarcoma with Van Gieson’s stain highlighting connective tissue. The classic alternating pattern of gliomatous (pink) and sarcomatous (yellow-brown) tissue is evident. Courtesy of Wikimedia Commons [author Marvin 101, https://commons.wikimedia.org/wiki/File:Gliosarcoma_Histopathology_200x_EVG.jpg].
-
This glioblastoma is composed of large epithelioid cells that are immunoreactive for glial fibrillary acidic protein (GFAP) (hematoxylin and eosin, 40× original magnification). Courtesy of Roger E McLendon, MD.
-
This typical untreated glioblastoma, here with the classic "butterfly" configuration, is a necrotic hemorrhagic mass. Courtesy of Wikimedia Commons [author Rodney D McComb, MD and The Armed Forces Institute of Pathology, https://commons.wikimedia.org/wiki/File:Glioblastoma_multiforme.jpg].









