Practice Essentials
Upper respiratory tract infection (URI) represents the most common acute illness evaluated in the outpatient setting. URIs range from the common cold—typically a mild, self-limited, catarrhal syndrome of the nasopharynx—to life-threatening illnesses such as epiglottitis (see the image below).
 Lateral neck radiograph demonstrates epiglottitis. Courtesy of Marilyn Goske, MD, Cleveland Clinic Foundation.
Lateral neck radiograph demonstrates epiglottitis. Courtesy of Marilyn Goske, MD, Cleveland Clinic Foundation.
Signs and symptoms
Details of the patient's history aid in differentiating a common cold from conditions that require targeted therapy, such as group A streptococcal pharyngitis, bacterial sinusitis, and lower respiratory tract infections. Clinical manifestations of these conditions, as well as allergy, show significant overlap.
Viral nasopharyngitis
Patients with the common cold may have a paucity of clinical findings despite notable subjective discomfort. Findings may include the following:
-
Nasal mucosal erythema and edema are common
-
Nasal discharge: Profuse discharge is more characteristic of viral infections than bacterial infections; initially clear secretions typically become cloudy white, yellow, or green over several days, even in viral infections
-
Foul breath
-
Fever: Less common in adults but may be present in children with rhinoviral infections
Group A streptococcal pharyngitis The following physical findings suggest a high risk for group A streptococcal disease [1] :
-
Erythema, swelling, or exudates of the tonsils or pharynx
-
Temperature of 38.3°C (100.9°F) or higher
-
Tender anterior cervical nodes (≥1 cm)
-
Absence of conjunctivitis, cough, and rhinorrhea, which are symptoms that may suggest viral illness [2]
Acute bacterial rhinosinusitis In children, acute bacterial sinusitis is defined as a URI with any of the following [3] :
-
Persistent nasal discharge (any type) or cough lasting 10 days or more without improvement
-
Worsening course (new or worse nasal discharge, cough, fever) after initial improvement
-
Severe onset (fever of 102° or greater with nasal discharge) for at least 3 consecutive days
In older children and adults, symptoms (eg, pain, pressure) tend to localize to the affected sinus.
Epiglottitis
This condition is more often found in children aged 1-5 years, who present with a sudden onset of the following symptoms:
-
Sore throat
-
Drooling, difficulty or pain during swallowing, globus sensation of a lump in the throat
-
Muffled dysphonia or loss of voice
-
Dry cough or no cough, dyspnea
-
Fever, fatigue or malaise (may be seen with any URI)
-
Tripod or sniffing posture
Laryngotracheitis and laryngotracheobronchitis
-
Nasopharyngitis often precedes laryngitis and tracheitis by several days
-
Swallowing may be difficult or painful
-
Patients may experience a globus sensation of a lump in the throat
-
Hoarseness or loss of voice is a key manifestation of laryngeal involvement
Features of whooping cough (pertussis) are as follows:
-
The classic whoop sound [4] is an inspiratory gasping squeak that rises in pitch, typically interspersed between hacking coughs
-
The whoop is more common in children
-
Coughing often comes in paroxysms of a dozen coughs or more at a time and is often worst at night
The 3 classic phases of whooping cough are as follows:
-
Catarrhal (7-10 days) with predominantly URI symptoms
-
Paroxysmal (1-6 weeks) with episodic cough
-
Convalescent (7-10 days) of gradual recovery [5]
See Clinical Presentation for more detail.
Diagnosis
Tests of nasopharyngeal specimens for specific pathogens are helpful when targeted therapy depends on the results (eg, group A streptococcal infection, gonococcus, pertussis). Specific bacterial or viral testing is also warranted in other selected situations, such as when patients are immunocompromised, during certain outbreaks, or to provide specific therapy to contacts.
Diagnosis of specific disorders is based on the following:
-
Group A streptococcal infection: Clinical findings or a history of exposure to a case, supported by results of rapid-detection assays and cultures (positive rapid antigen detection tests do not necessitate a backup culture)
-
Acute bacterial rhinosinusitis: Laboratory studies are generally not indicated; Computed tomography (CT) scanning or other sinus imaging may be appropriate if symptoms persist despite therapy or if complications (eg, extension of disease into surrounding tissue) are suspected
-
Influenza: Rapid tests have over 70% sensitivity and more than 90% specificity
-
Mononucleosis: Heterophile antibody testing (eg, Monospot)
-
Herpes simplex virus infection: Cell culture or polymerase chain reaction (PCR) assay
-
Pertussis: Rapid tests; culture of a nasopharyngeal aspirate (criterion standard)
-
Epiglottitis: Direct visualization by laryngoscopy, performed by an otorhinolaryngologist
-
Gonococcal pharyngitis: Throat culture for Neisseria gonorrhoeae
Blood cultures are typically appropriate only in hospitalized patients with suspected systemic illness. Imaging studies are warranted in patients with suspected mass lesions (eg, peritonsillar abscess, intracranial suppurative lesions).
See Workup for more detail.
Management
Symptom-basedtherapy represents the mainstay of URI treatment in immunocompetent adults. Antimicrobial or antiviral therapy is appropriate in selected patients.
Epiglottitis
-
Immediately admit the patient to the nearest hospital
-
Avoid instrumentation; insertion of tongue depressors or other instruments may provoke airway spasm and precipitate respiratory compromise
-
Monitor for respiratory fatigue, visually and with continuous pulse oximetry
-
Administer oxygen according to pulse oximetry results
-
Have equipment and personnel available for immediate intubation if necessary
-
Start intravenous (IV) antibiotics after collecting culture specimens
-
Empiric coverage for Haemophilus influenzae is appropriate; common choices include ceftriaxone or other third-generation cephalosporins, cefuroxime, and cefamandole
-
Correct volume deficits with IV fluids; avoid sedatives
Laryngotracheitis
-
Hospitalization may be necessary, especially in infants and young children who have hypoxemia, volume depletion, a risk of airway compromise, or respiratory fatigue
-
Mild cases of croup (ie, laryngotracheobronchitis) may be managed at home with moist air inhalation
-
Hospitalized patients require monitoring for respiratory fatigue, visually and with continuous pulse oximetry
-
Expertise for immediate intubation and access to the necessary equipment are required if respiratory failure is a possibility
-
Administer humidified oxygen to all hypoxemic patients. In patients who do not require oxygen therapy, a cool-mist humidifier may be used
-
IV or oral glucocorticoids are commonly used to reduce symptoms and shorten hospitalization in patients with moderate to severe croup
-
Inhaled racemic epinephrine may temporarily dilate the airways
Rhinosinusitis
-
Most cases of acute rhinosinusitis, including mild and moderate bacterial sinusitis, resolve without antibiotics [6]
-
Consider antibiotic treatment if symptoms persist without improving for 10 or more days, or if symptoms are severe or worsening during a period of 3-4 days or longer [7]
-
Give first-line antibiotics for 5-7 days in most adults; for 10-14 days in children
-
Begin treatment with an agent that most narrowly covers likely pathogens, including Streptococcus pneumoniae, nontypeable H influenzae, and Moraxella catarrhalis
-
Initial first-line options include amoxicillin/clavulanate
-
Alternatives in penicillin-allergic patients are doxycycline and respiratory fluoroquinolones (eg, levofloxacin, moxifloxacin)
-
In patients who worsen or do not improve after 3-5 days of empirical therapy, consider resistant pathogens, structural abnormality, or noninfectious etiology
-
Adjunctive therapy for adults includes nasal saline irrigation and intranasal steroids
Group A streptococcal disease
-
Oral penicillin or amoxicillin for 10 days for patients without an allergy to penicillin
-
If compliance is a concern, consider a single IM injection of benzathine penicillin G
-
A first-generation cephalosporin may be used in patients with non-anaphylactic penicillin allergy
-
Options for penicillin-allergic patients include clindamycin or clarithromycin for 10 days or azithromycin for 5 days [2]
See Treatment and Medication for more detail.
Background
Upper respiratory tract infection (URI) represents the most common acute illness evaluated in the outpatient setting. URIs range from the common cold—typically a mild, self-limited, catarrhal syndrome of the nasopharynx—to life-threatening illnesses such as epiglottitis.
Viruses account for most URIs (see Etiology). Appropriate management in these cases may consist of reassurance, education, and instructions for symptomatic home treatment. Diagnostic tests for specific agents are helpful when targeted URI therapy depends on the results (see Workup). Bacterial primary infection or superinfection may require targeted therapy (see Treatment).
The upper respiratory tract includes the sinuses, nasal passages, pharynx, and larynx, which serve as gateways to the trachea, bronchi, and pulmonary alveolar spaces. Rhinitis, pharyngitis, sinusitis, epiglottitis, laryngitis, and tracheitis are specific manifestations of URIs. Further information can be found in the Medscape Reference articles Acute Laryngitis, Acute Sinusitis, Allergic Rhinitis, Bacterial Tracheitis, Croup, Epiglottitis, Pharyngitis, and Viral Pharyngitis.
Common URI terms are defined as follows:
-
Rhinitis: Inflammation of the nasal mucosa
-
Rhinosinusitis or sinusitis: Inflammation of the nares and paranasal sinuses, including frontal, ethmoid, maxillary, and sphenoid
-
Nasopharyngitis (rhinopharyngitis or the common cold): Inflammation of the nares, pharynx, hypopharynx, uvula, and tonsils
-
Pharyngitis: Inflammation of the pharynx, hypopharynx, uvula, and tonsils
-
Epiglottitis (supraglottitis): Inflammation of the superior portion of the larynx and supraglottic area
-
Laryngitis: Inflammation of the larynx
-
Laryngotracheitis: Inflammation of the larynx, trachea, and subglottic area
-
Tracheitis: Inflammation of the trachea and subglottic area
Pathophysiology
URIs involve direct invasion of the mucosa lining the upper airway. Inoculation of bacteria or viruses occurs when a person’s hand comes in contact with pathogens and the person then touches the nose or mouth or when a person directly inhales respiratory droplets from an infected person who is coughing or sneezing.
After inoculation, viruses and bacteria encounter several barriers, including physical, mechanical, humoral, and cellular immune defenses. Physical and mechanical barriers include the following:
-
Hair lining the nose filters and traps some pathogens
-
Mucus coats much of the upper respiratory tract, trapping potential invaders
-
The angle resulting from the junction of the posterior nose to the pharynx causes large particles to impinge on the back of the throat
-
Ciliated cells lower in the respiratory tract trap and transport pathogens up to the pharynx; from there they are swallowed into the stomach
Adenoids and tonsils contain immune cells that respond to pathogens. Humoral immunity (immunoglobulin A) and cellular immunity act to reduce infections throughout the entire respiratory tract. Resident and recruited macrophages, monocytes, neutrophils, and eosinophils coordinate to engulf and destroy invaders.
A host of inflammatory cytokines mediates the immune response to invading pathogens. Normal nasopharyngeal flora, including various staphylococcal and streptococcal species, help to defend against potential pathogens. Patients with suboptimal humoral and phagocytic immune function are at increased risk for contracting a URI, and they are at increased risk for a severe or prolonged course of disease.
Inflammation (chronic or acute) from allergy predisposes to URI. Children with allergy are particularly subject to frequent URIs.
Infection
Person-to-person spread of viruses accounts for most URIs. Household and child care settings can serve as reservoirs for infection. Bacterial infections may develop de novo or as a superinfection of a viral URI.
Viral agents occurring in URIs include a vast number of serotypes, which undergo frequent changes in antigenicity, posing challenges to immune defense. Pathogens resist destruction by a variety of mechanisms, including the production of toxins, proteases, and bacterial adherence factors, as well as the formation of capsules that resist phagocytosis.
Incubation times before the appearance of symptoms vary among pathogens. Rhinoviruses and group A streptococci may incubate for 1-5 days, influenza and parainfluenza may incubate for 1-4 days, and respiratory syncytial virus (RSV) may incubate for a week. Pertussis typically incubates for 7-10 days, or even as long as 21 days, before causing symptoms. Diphtheria incubates for 1-10 days. The incubation period of Epstein-Barr virus (EBV) is 4-6 weeks.
Most symptoms of URIs—including local swelling, erythema, edema, secretions, and fever—result from the inflammatory response of the immune system to invading pathogens and from toxins produced by pathogens.
An initial nasopharyngeal infection may spread to adjacent structures, resulting in the following:
-
Sinusitis
-
Otitis media
-
Epiglottitis
-
Laryngitis
-
Tracheobronchitis
-
Pneumonia
Inflammatory narrowing at the level of the epiglottis and larynx may result in a dangerous compromise of airflow, especially in children, in whom a small reduction in the luminal diameter of the subglottic larynx and trachea may be critical. Beyond childhood, laryngotracheal inflammation may also pose serious threats to individuals with congenital or acquired subglottic stenosis.
Susceptibility
Genetic susceptibility is involved in determining which patients have more severe disease courses than others. There are some recognized candidate gene polymorphisms with known functional changes in genes that may lead to immunosuppression. [8] It has also been shown that host immunogenetic variation plays a role in the immune response to H1N1 and H5N1 viruses, thereby influencing disease severity and outcome in influenza caused by these viruses. [9, 10]
Etiology
Most URIs are viral in origin. Typical viral agents that cause URIs include the following:
-
Rhinoviruses
-
Coronaviruses
-
Adenoviruses
-
Coxsackieviruses
For the most part, similar agents cause URI in adults and children; however, Moraxella catarrhalis and bocavirus cause URIs more commonly in children than in adults.
Nasopharyngitis
Of the more than 200 viruses known to cause the symptoms of the common cold, the principal ones are as follows:
-
Rhinoviruses: These cause approximately 30-50% of colds in adults; they grow optimally at temperatures near 32.8°C (91°F), which is the temperature inside the human nares
-
Coronaviruses: While they are a significant cause of colds, exact case numbers are difficult to determine because, unlike rhinoviruses, coronaviruses are difficult to culture in the laboratory
-
Enteroviruses, including coxsackieviruses, echoviruses, and others
Other viruses that account for many URIs include the following:
-
Adenoviruses
-
Orthomyxoviruses (including influenza A and B viruses)
-
Paramyxoviruses (eg, parainfluenza virus [PIV])
-
RSV
-
EBV
-
Human metapneumovirus (hMPV)
-
Bocavirus: Commonly associated with nasopharyngeal symptoms in children [11]
Unidentified, but presumably viral, pathogens account for more than 30% of common colds in adults. In addition, varicella, rubella, and rubeola infections may manifest as nasopharyngitis before other classic signs and symptoms develop.
Pharyngitis
This is most often viral in origin. Recognition of group A streptococcal pharyngitis is vital because serious complications may follow untreated disease.
Viral causes of pharyngitis include the following:
-
Adenovirus: May also cause laryngitis and conjunctivitis
-
Influenza viruses
-
Coxsackievirus
-
Herpes simplex virus (HSV)
-
EBV (infectious mononucleosis)
-
Cytomegalovirus (CMV)
Bacterial causes of pharyngitis include the following:
-
Group A streptococci (approximately 5-15% of all cases of pharyngitis in adults; 20-30% in children) [2]
-
Group C and G streptococci
-
Neisseria gonorrhoeae
-
Arcanobacterium (Corynebacterium) hemolyticum
-
Corynebacterium diphtheriae
-
Atypical bacteria (eg, Mycoplasma pneumoniae and Chlamydia pneumoniae; absent lower respiratory tract disease, the clinical significance of these pathogens is uncertain)
-
Anaerobic bacteria
Rhinosinusitis
Rhinosinusitis in an immunocompetent person is typically related to an uncomplicated viral URI. Viral causes are similar to those of viral nasopharyngitis and include the following:
-
Rhinovirus
-
Enterovirus
-
Coronavirus
-
Influenza A and B virus
-
PIV
-
RSV
-
Adenovirus
Bacterial causes are similar to those seen in otitis media. Bacterial pathogens isolated from maxillary sinus aspirates of patients with acute bacterial rhinosinusitis include the following [7] :
-
Streptococcus pneumoniae: 38% in adults, 21-33% in children
-
Haemophilus influenzae: 36% in adults, 31-32% in children
-
Moraxella catarrhalis: 16% in adults; 8-11% in children
-
Staphylococcus aureus: 13% in adults, 1% in children
Other pathogens include group A streptococci and other streptococcal species. Uncommon causes include C pneumoniae, Neisseria species, anaerobes, and gram-negative rods.
Nosocomial sinusitis often involves pathogens that colonize the upper respiratory tract and migrate into the sinuses. Prolonged endotracheal intubation places patients at increased risk for nosocomial sinusitis. Methicillin-resistant S aureus (MRSA) is less common than sensitive staphylococci. [7] Gram-negative bacilli (eg, Escherichia coli,Pseudomonas aeruginosa) are other causes.
Aspergillus species are the leading causes of noninvasive fungal sinusitis. Although fungi are part of the normal flora of the upper airways, they may cause acute sinusitis in patients with immunocompromise or diabetes mellitus.
Epiglottitis
This is a bacterial infection. In the vast majority of children, H influenzae type b (Hib) is isolated from blood or epiglottal cultures. Since the routine use of the Hib conjugate vaccine began in 1990, case rates in children younger than 5 years have declined by more than 95%. The prevalence of invasive Hib disease is approximately 1.3 cases per 100,000 children. [12] Rates in adults have remained low and stable; Alaskan Natives have the highest rates of disease.
Other bacteria, found more commonly in adults than in children, include group A streptococci, S pneumoniae, and M catarrhalis. In adults, cultures are most likely to be negative.
Laryngotracheitis
Croup, or laryngotracheobronchitis, is typically caused by PIV type 1, 2, or 3. PIVs account for up to 80% of croup cases. PIV type 1 is the leading cause of croup in children. [13] Other viruses include influenza viruses and RSV. Uncommon causes include hMPV, adenovirus, rhinovirus, enterovirus (including coxsackievirus and enteric cytopathic human orphan [ECHO] viruses), and measles virus.
Approximately 95% of all cases of whooping cough are caused by the gram-negative rod Bordetella pertussis. The remaining cases result from B parapertussis.
Other forms of laryngitis and laryngotracheitis are typically caused by viruses similar to those that cause nasopharyngitis, including rhinovirus, coronavirus, adenovirus, influenza virus, parainfluenza virus, and RSV. Candida species may cause laryngitis in immunocompromised hosts.
Bacterial laryngitis is far less common than viral laryngitis. [14] Bacterial causes include the following:Group A streptococci
-
Corynebacterium diphtheriae, an aerobic gram-positive rod that may infect only the larynx or may represent an extension of nasopharyngeal infection
-
Chlamydia pneumoniae
-
Mycoplasma pneumoniae
-
Moraxella catarrhalis
-
H influenzae
-
S aureus
-
Mycobacterium tuberculosis: Tuberculosis has been reported in renal transplant recipients and human immunodeficiency virus (HIV) ̶ infected patients
Risk factors for URIs
Risk factors for contracting a URI include the following:
-
Contact: Close contact with small children who frequent group settings, such as school or daycare, increases the risk of URI, as does the presence of URI in the household or family
-
Inflammation: Inflammation and obstruction from allergic rhinitis or asthma can predispose to infections
-
Travel: The incidence of contracting a URI is increased because of exposure to large numbers of individuals in closed settings
-
Smoking and exposure to second-hand smoke: These may alter mucosal resistance to URI
-
Immunocompromise that affects cellular or humoral immunity: Weakened immune function may result from splenectomy, HIV infection, use of corticosteroids, immunosuppressive treatment after stem cell or organ transplantation, multiple medical problems, or common stress; cilia dyskinesia syndrome and cystic fibrosis also predispose individuals to URIs
-
Anatomic changes due to facial dysmorphisms, previous upper airway trauma, and nasal polyposis
-
Carrier state: Although some people are chronic carriers of group A streptococci, repeated URIs in such patients may be viral in origin [2]
Epidemiology
URIs are the most common infectious illness in the general population and are the leading cause of missed days at work or school. They represent the most frequent acute diagnosis in the office setting. [15]
Nasopharyngitis
The incidence of the common cold varies by age. Rates are highest in children younger than 5 years. Children who attend school or day care are a large reservoir for URIs, and they transfer infection to the adults who care for them. In the first year after starting at a new school or day care, children experience more infections, as do their family members. Children have about 3-8 viral respiratory illnesses per year, adolescents and adults have approximately 2-4 colds annually, and people older than 60 years have fewer than 1 cold per year.
Pharyngitis
Acute pharyngitis accounts for 1% of all ambulatory office visits. [15] The incidence of viral and bacterial pharyngitis peaks in children aged 4-7 years.
Rhinosinusitis
Sinusitis is common in persons with viral URIs. Transient changes in the paranasal sinuses are noted on computed tomography (CT) scans in more than 80% of patients with uncomplicated viral URIs. [16] However, bacterial rhinosinusitis occurs as a complication in only about 2% of persons with viral URIs. [17]
Epiglottitis
The occurrence of epiglottitis has decreased dramatically in the United States and other developed nations since the introduction of Hib vaccine. A Swedish study documented that the Hib vaccination program was associated with a decrease in the overall annual incidence of acute epiglottitis from 4.5 cases to 0.98 cases per 100,000 population; the incidence decreased in children and adults. However, the annual incidence of pneumococcal epiglottitis in adults increased from 0.1 to 0.28 cases per 100,000 population over the same period. [18]
Laryngitis and laryngotracheitis
Croup, or laryngotracheobronchitis, may affect people of any age but usually occurs in children aged 6 months to 6 years. The peak incidence is in the second year of life. Thereafter, the enlarging caliber of the airway reduces the severity of the manifestations of subglottic inflammation.
Vaccination has dramatically reduced rates of pertussis. However, the incidence of whooping cough in the United States has increased steadily since 2007, reaching approximately 9 cases per 100,000 population in 2010. Rates of pertussis are highest in infants below age 1 year; adolescents and adults accounted for approximately 44% of the 27,550 cases of pertussis reported in the United States in 2010. [19]
Worldwide, pertussis has an estimated incidence of 48.5 million cases and causes nearly 295,000 deaths per year. In low-income countries, the case-fatality rate among infants may be as high as 4%. [20]
Although pertussis is a nationally notifiable disease in the United States, many cases likely go undiagnosed and unreported. On the other hand, challenges in laboratory diagnosis and overreliance on polymerase chain reaction (PCR) assays have resulted in reports of respiratory illness outbreaks mistakenly attributed to pertussis. [21]
Occurrence rate of selected pathogens
Group A streptococcal bacteria cause approximately 5-15% of all pharyngitis infections, [2] accounting for several million cases of streptococcal pharyngitis each year. This infection is rarely diagnosed in children younger than 2 years.
Influenza affects approximately 5-20% of the US population during each flu season. [22] Early presentations include symptoms of URI.
EBV infection affects as many as 95% of American adults by age 35-40 years. Childhood EBV infection is indistinguishable from other transient childhood infections. Approximately 35-50% of adolescents and young adults who contract EBV infection have mononucleosis. [23]
Diphtheria rates fell dramatically in the United States after the advent of diphtheria vaccine. Since 1980, the prevalence of diphtheria has been approximately 0.001 case per 100,000 population. A confirmed case of the disease has not been reported in the United States since 2003. [24] However, diphtheria remains endemic in developing countries.
Seasonality
Although URIs may occur year round, in the United States most colds occur during fall and winter. Beginning in late August or early September, rates of colds increase over several weeks and remain elevated until March or April. [25] Epidemics and mini-epidemics are most common during cold months, with a peak incidence from late winter to early spring.
Cold weather results in more time spent indoors (eg, at work, home, school) and close exposure to others who may be infected. Humidity may also affect the prevalence of colds, because most viral URI agents thrive in the low humidity that is characteristic of winter months. Low indoor air moisture may increase friability of the nasal mucosa, increasing a person's susceptibility to infection.
Laryngotracheobronchitis, or croup, occurs in fall and winter. Seasonality does not affect rates of epiglottitis.
The figure below illustrates the peak incidences of various agents by season. Rhinoviruses, which account for a substantial percentage of URIs, are most active in spring, summer, and early autumn. Coronaviral URIs manifest primarily in the winter and early spring. Enteroviral URIs are most noticeable in summer and early fall, when other URI pathogens are at a nadir. Adenoviral respiratory infections can occur throughout the year but are most common in the late winter, spring, and early summer.
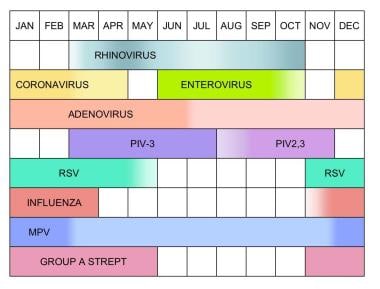 Seasonal variation of selected upper respiratory tract infection pathogens. PIV is parainfluenza virus, RSV is respiratory syncytial virus, MPV is metapneumovirus, and Group A Strept is group A streptococcal disease.
Seasonal variation of selected upper respiratory tract infection pathogens. PIV is parainfluenza virus, RSV is respiratory syncytial virus, MPV is metapneumovirus, and Group A Strept is group A streptococcal disease.
Seasonal influenza typically lasts from November until March. Some PIVs have a biennial pattern. The patterns for human PIV types 1-3 are as follows:
-
Human PIV type 1: Currently produces autumnal outbreaks in the United States during odd-numbered years; the leading cause of croup in children
-
Human PIV type 2: May cause annual or biennial fall outbreaks
-
Human PIV type 3: Peak activity is during the spring and early summer months; however, the virus may be isolated throughout the year. [13]
Human metapneumovirus (hMPV) infection may also occur year round, although the infection rates peak between December and February.
Race- and sex-related demographics
No notable racial difference is observed with URIs. However, Alaskan Natives have rates of Hib disease higher than those of other groups. [12]
Sexual disparities among URIs are as follows:
-
Rhinitis: Hormonal changes during the middle of the menstrual cycle and during pregnancy may produce hyperemia of the nasal and sinus mucosa and increase nasal secretions; URI may be superimposed over these baseline changes and may increase the intensity of symptoms in some women
-
Nasopharyngitis: The common cold occurs frequently in women, especially those aged 20-30 years [25] ; this frequency may represent increased exposure to small children, who represent a large reservoir for URIs, but hormonal effects on the nasal mucosa may also play a role
-
Epiglottitis: A male predominance is reported, with a male-to-female ratio of approximately 3:2
-
Laryngotracheobronchitis, or croup: More common in boys than in girls, with a male-to-female ratio of approximately 3:2
Age-related demographics
The incidence of the common cold varies by age. Rates are highest in children younger than 5 years. Children have approximately 3-8 viral respiratory illnesses per year, while adolescents and adults have approximately 2-4 colds a year, and people older than 60 years have fewer than 1 cold per year.
The age-related occurrence of other infections is as follows:
-
Viral and bacterial pharyngitis: Peaks in children aged 4-7 years.
-
Epiglottitis: Typically occurs in children aged 2-7 years and has a peak incidence in those aged 3 years
-
Laryngotracheobronchitis (croup): As previously stated, it may affect people of any age but usually occurs in children aged 6 months to 6 years; the peak incidence is in the second year of life
Prognosis
URIs cause people to spend time away from their usual daily activities, but alone, these infections rarely cause permanent sequelae or death. URIs may, however, serve as a gateway to infection of adjacent structures, resulting in the following infections (and others, as well):
-
Otitis media
-
Bronchitis
-
Bronchiolitis
-
Pneumonia
-
Sepsis
-
Meningitis
-
Intracranial abscess
Serious complications may result in clinically significant morbidity and rare deaths.
Nasopharyngitis
A common cold may last up to 14 days, with symptoms averaging 7-11 days in duration. [17]
Fever, sneezing, and sore throat typically resolve early, whereas cough and nasal discharge are among the symptoms that last longest.
Attendance at day care may affect the duration of symptoms in young children. In one study, the duration of viral URIs ranged from 6.6 days for children aged 1-2 years in home care to 8.9 days for children younger than 1 year who were in day care. Young children in day care were also more likely to have protracted respiratory symptoms lasting more than 15 days. [26]
Most patients with influenza recover within a week, although cough, fatigue, and malaise may persist for up to 2 weeks. For newborns, elderly persons, and patients with chronic medical conditions, the flu may be life threatening. More than 200,000 people per year are hospitalized because of complications of the flu, with 0.36 deaths per 100,000 patients occurring annually. [27] Influenza may be followed by bacterial superinfection.
Pharyngitis
Viral pharyngitis typically resolves in 1-2 weeks, but immunocompromised persons may have a more severe course.
Untreated group A streptococcal pharyngitis can result in the following:
-
Acute rheumatic fever
-
Acute glomerulonephritis
-
Peritonsillar abscess
-
Toxic shock syndrome
-
Impetigo
-
Cellulitis or abscess
-
Otitis
-
Sinusitis
-
Conjunctivitis
-
Bronchitis
Mortality from group A streptococcal pharyngitis is rare, but serious morbidity or death may result from one of its complications.
Streptococcal pharyngitis without complications rarely poses significant risk for morbidity. However, retropharyngeal, intraorbital, or intracranial abscesses may cause serious sequelae. The risk of mortality is significant in patients who progress to streptococcal toxic shock syndrome, which is characterized by multiorgan failure and hypotension.
In patients with penicillin-sensitive streptococcal pharyngitis, symptomatic improvement is expected within 24-72 hours if antibiotic treatment is started in the first 24 hours after onset. Treatment failures are common and are mainly attributed to poor adherence, antibiotic resistance, and untreated close contacts, usually within the household or family.
A chronic carrier state may develop with group A streptococcal infection. Eradicating the pathogen is difficult in these cases; however, carriers without active symptoms are unlikely to spread group A streptococci, and they are at low risk for developing rheumatic fever.
Mononucleosis
With infectious mononucleosis from EBV, complete resolution of symptoms may take up to 2 months. Acute symptoms rarely last more than 4 months. EBV typically remains dormant throughout the patient's life. Reactivation of the virus is not usually symptomatic.
Rhinosinusitis
The prognosis is generally favorable for acute rhinosinusitis, and many cases appear to resolve even without antibiotic therapy. As many as 70% of immunocompetent adults with rhinosinusitis begin to improve within 2 weeks of presentation without antibiotics. With antibiotics, up to 85% have improvement at 2 weeks. Complete resolution may take weeks to months.
Sinusitis itself is rarely life threatening, but it can lead to serious complications if the infection extends into surrounding deep tissue, including the following:
-
Orbital cellulitis
-
Subperiosteal abscess
-
Orbital abscess
-
Frontal and maxillary osteomyelitis
-
Subdural abscess
-
Meningitis
-
Brain abscess
Epiglottitis
Epiglottitis poses a risk of death due to sudden airway obstruction and other complications, including septic arthritis, meningitis, empyema, and mediastinitis. In adults, epiglottitis has a fatality rate of approximately 1%.
The prognosis is favorable with appropriate airway management, and most patients noticeably improve within 24-48 hours after antibiotics are started. Rarely, cases of epiglottitis may recur. Recurrent symptoms raise concern about potential underlying disorders, such as rheumatic conditions, sarcoidosis, and occult malignancy.
Laryngitis and laryngotracheitis
With croup, laryngotracheobronchitis typically begins to improve within 3-4 days. Recovery is usually complete. However, patients may have a recurrence, including during the same season.
Pertussis (whooping cough) leads to hospitalization in more than half of infants younger than 12 months and particularly in infants younger than 6 months. Infants and young children are most susceptible to severe courses that include respiratory compromise.
Of infants who are hospitalized with pertussis, approximately 50% have apnea, 20% develop pneumonia, 1% have seizures, 1% die, and 0.3% have encephalopathy. [28] Recovery from whooping cough is typically complete. However, paroxysms of coughing may last for several weeks.
Complications
Most URIs are self-limited and resolve completely. However, a variety of conditions may complicate a URI. Fluid loss may occur in patients unable to tolerate adequate oral intake because of upper airway inflammation or may result from fever. Otitis media may complicate 5% of colds in children and up to 2% of colds in adults [29]
Airway hyperreactivity may increase after a URI, resulting in new or exacerbated asthma. Cough asthma, wherein a cough is the predominant manifestation of reactive airways disease, may mimic ongoing infection. This may be diagnosed with pulmonary function testing.
A postinfectious cough is defined as coughing that persists 3-8 weeks after the onset of a URI in the absence of other clearly defined causes. Exacerbations of chronic obstructive pulmonary disease, including emphysema and chronic bronchitis, may occur during and after a URI. Upper airways cough syndrome (post-nasal drip) may result from upper airway secretions dripping onto the pharynx. Epistaxis may also occur.
Lower respiratory tract disease and sepsis represent serious complications, especially in patients with immunocompromise. Lower respiratory tract disease should be considered when symptoms such as fever, cough, sputum, and malaise worsen progressively or after initial transient improvement. Tachypnea and dyspnea are also signs of lower respiratory involvement.
Viral infection and resulting inflammation may make an individual susceptible to concomitant or sequential infection with a bacterial agent. Streptococcus pneumoniae, Staphylococcus aureus, H influenzae, and Streptococcus pyogenes are common superinfecting agents. Meningococci may cause superinfection with influenzal infections.
Inflammation of the larynx and trachea area may lead to airway compromise, especially in children and in patients with narrowed airways due to congenital or acquired subglottic stenosis. The work of breathing during epiglottitis or laryngotracheitis may lead to respiratory failure. Sleep apnea may occur from hypertrophied tonsils.
Deep tissue infection may occur by extension of the infection into the orbit, middle ear, cranium, or other areas. Peritonsillar abscess (quinsy) may complicate bacterial pharyngitis, leading to difficulty swallowing and pain radiating to the ear. Retropharyngeal abscess may also complicate pharyngitis. Lemierre syndrome is an extension of pharyngitis that leads to a suppurative thrombophlebitis of the internal jugular vein; septic thromboemboli may then spread throughout the body.
Complications of sinusitis include the following:
-
Orbital cellulitis
-
Subperiosteal abscess
-
Orbital abscess
-
Mastoiditis
-
Frontal or maxillary osteomyelitis
-
Subdural abscess
-
Cavernous sinus thrombosis
-
Brain abscess
Suspect a deep tissue infection when a patient has orbital or periorbital swelling, proptosis, impaired extraocular movements, or impaired vision. Signs of increased intracranial pressure (eg, papilledema, altered mental status, neurologic findings) may suggest intracranial involvement.
Encephalitis, meningitis, or subarachnoid hemorrhage may follow a URI. Osteomyelitis may complicate persistent or recurrent sinusitis. Osteomyelitis may affect the orbital plate, frontal bone, or sphenoid bone. Mucoceles are expanding cystic defects of the paranasal sinuses that may result from prolonged sinusitis. Epiglottic abscess may result from epiglottitis.
Lymphadenitis may follow or accompany URI. Guillain-Barré syndrome may manifest as an ascending polyneuropathy a few days or weeks after a URI. In children or adolescents, the use of aspirin during a viral infection may rarely cause Reye syndrome. Aspirin is contraindicated for the management of fevers in children or adolescents.
URI, especially with fever, may increase the work of the heart, adding strain to persons with suboptimal cardiovascular status, and can lead to cardiovascular decompensation. Myositis or pericarditis may result from viral infection.
Hyperglycemia may occur during a URI in patients with diabetes. Rib fracture may be seen following an episode of severe coughing, such as that associated with whooping cough. Hernia may develop following an episode of severe coughing.
Cutaneous complications such as rash, cellulitis, and toxic shock syndrome may occur with group A streptococcus. This pathogen can also be associated with glomerulonephritis, acute rheumatic fever, and PANDAS syndrome (Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections).
Hemoptysis suggests the possibility of tuberculosis. A tuberculin skin test, chest radiography, or both are appropriate in these patients.
Complications of specific conditions
Complications of group A streptococcal disease
Group A streptococcal pharyngitis is of special concern because its complications include streptococcal toxic shock syndrome, acute rheumatic fever (ARF), acute glomerulonephritis, and scarlet fever, as well as cutaneous infections. In addition, this pathogen is readily transmissible, especially in households, families, and other intimate groups.
ARF affects approximately 3% of patients with strep throat, primarily occurring in persons aged 6-20 years. The condition develops approximately 2-4 weeks after streptococcal pharyngitis occurs, and it may last several months. Signs of rheumatic fever include arthritis, fever, and valvular disease. Uncommon features include an expanding truncal exanthem (erythema marginata), subcutaneous nodules, and chorea.
Poststreptococcal glomerulonephritis can affect persons of any age group, but it is most common in children aged 3-7 years. Boys are affected slightly more often than girls. Patients with glomerulonephritis may have loss of appetite, lethargy, dull back pain, and dark urine. Blood pressure may be elevated, and edema may occur.
Scarlet fever is a self-limited exanthem that spreads from the chest and abdomen to the entire body. Tiny red papules create a rough skin texture similar to that of sandpaper. The rash is typically blanching. Although it commonly affects the face, circumoral pallor is present. During recovery, the skin on the fingers and toes peels. Streptococcal toxic shock syndrome may also occur, affecting skin and mucosa.
PANDAS is a rare syndrome in children and adolescents, who experience sudden onset or worsening of obsessive-compulsive disorder following streptococcal infection. Associated manifestations include tics and a variety of neuropsychiatric symptoms. [30]
Complications of mononucleosis
Complications can include the following:
-
Splenic rupture
-
Hepatitis
-
Guillain-Barré syndrome
-
Encephalitis
-
Hemolytic anemia
-
Agranulocytosis
-
Myocarditis
-
Burkitt lymphoma
-
Nasopharyngeal carcinoma
-
Rash (with concomitant use of ampicillin)
Complications of diphtheria
Complications may include airway obstruction, myocarditis, polyneuritis, thrombocytopenia, and proteinuria. Among patients who survive diphtheria, as many as 20% have permanent hearing loss or other long-term sequelae. [13]
Complications from pertussis
More than half of infants younger than 12 months who contract pertussis require hospitalization, especially those who are younger than 6 months. Complications of pertussis in hospitalized infants include the following [28] :
-
Apnea (50%)
-
Pneumonia (20%)
-
Seizures (1%)
-
Encephalopathy (0.3%)
-
Death (1%)
In addition, severe cough may result in rib fractures, hernia, incontinence, or subconjunctival hemorrhages.
Complications of influenza
These include the following:
-
Bacterial superinfection
-
Pneumonia
-
Volume depletion
-
Myositis
-
Pericarditis
-
Rhabdomyolysis
-
Encephalitis
-
Meningitis
-
Myelitis
-
Renal failure
-
Disseminated intravascular coagulation
As with any systemic infection, the flu poses a risk of worsening underlying medical conditions, such as heart failure, asthma, or diabetes. After influenzal infection, children may experience sinus problems or otitis media.
Patient Education
Address the patient's expectations about antibiotic therapy. Validate the patient's symptoms and their severity, listen to the concerns expressed, and educate the patient about possible consequences of inappropriate antibiotic use, including consequences affecting him/her and the community.
Many people hold misperceptions about the duration and intensity of symptoms associated with URI and about the benefits and risks of antibiotic therapy. Some are unaware that cold symptoms may last as long as 14 days. Some believe that antibiotics will help them to avoid serious disease and recover more quickly than without treatment.
Patients may expect to receive antibiotics solely based on the severity of their symptoms, and they may not appreciate the negative consequences of using antibiotics in viral disease. Negative results on a rapid strep test may provide reassurance about the appropriateness of supportive care.
Actively promote self-care, and outline a realistic time course for the resolution of symptoms. Reassure the patient about access to clinical care and follow-up in the event that symptoms progress. Briefly explore factors that may have contributed to the current infection, and address prevention for the future.
Patient satisfaction is less linked to antibiotic prescriptions and more linked to the quality of the physician-patient interaction. Reflecting understanding of the details of the patient's situation, expressing concern for the patient's well-being, explaining how recommendations are appropriately tailored to the individual's current condition, and providing reassurance are important to patient satisfaction.
Patients should be counseled on handwashing and proper methods of covering coughs and sneezes. Patients who smoke should receive smoking cessation encouragement and materials. When antibiotics are prescribed, patients should be instructed to complete the full course of antibiotic therapy.
Patients should be instructed to follow up when indicated or if symptoms worsen. Finally, patients with infectious mononucleosis should be instructed to avoid contact sports for 6 weeks because of the possibility of splenic rupture.
For patient education information, see the Headache and Migraine Center, as well as Sinus Infection and Sore Throat.
-
Seasonal variation of selected upper respiratory tract infection pathogens. PIV is parainfluenza virus, RSV is respiratory syncytial virus, MPV is metapneumovirus, and Group A Strept is group A streptococcal disease.
-
CT scan of the sinuses demonstrates maxillary sinusitis. The left maxillary sinus is completely opacified (asterisk), and the right has mucosal thickening (arrow). Courtesy of Omar Lababede, MD, Cleveland Clinic Foundation.
-
Lateral neck radiograph demonstrates epiglottitis. Courtesy of Marilyn Goske, MD, Cleveland Clinic Foundation.
-
Gonococcal pharyngitis. Image credit: CDC Public Health Image Library (Flumara NJ, Hart G).
-
Strep throat with petechiae. CDC Public Health Image Library (Eichenwald HF).
Tables
Symptom |
Allergy |
URI |
Influenza |
Itchy, watery eyes |
Common |
Rare; conjunctivitis may occur with adenovirus |
Soreness behind eyes, sometimes conjunctivitis |
Nasal discharge |
Common |
Common |
Common |
Nasal congestion |
Common |
Common |
Sometimes |
Sneezing |
Very common |
Very common |
Sometimes |
Sore throat |
Sometimes (postnasal drip); itchy throat |
Very common |
Sometimes |
Cough |
Sometimes |
Common, mild to moderate, hacking cough |
Common, dry cough, can be severe |
Headache |
Sometimes, facial pain |
Rare |
Common |
Fever |
Never |
Rare in adults, possible in children |
Very common, 100-102°F or higher (in young children), lasting 3-4 days; may have chills |
Malaise |
Sometimes |
Sometimes |
Very common |
Fatigue, weakness |
Sometimes |
Sometimes |
Very common, can last for weeks, extreme exhaustion early in course |
Myalgias |
Never |
Slight |
Very common, often severe |
Duration |
Weeks |
3-14 days |
7 days, followed by additional days of cough and fatigue |

What would you like to print?
- Overview
- Presentation
- DDx
- Workup
- Treatment
- Approach Considerations
- Epiglottitis
- Laryngotracheitis
- Rhinosinusitis
- Group A Streptococcal Disease
- Herpetic or Gonococcal Pharyngitis
- Other Conditions That May Warrant Specific Treatment
- Patients With Immunocompromise
- Surgical Care
- Symptomatic, Nonpharmacologic Self-Care
- Symptomatic, Pharmacologic Therapy
- Diet
- Activity
- Deterrence/Prevention
- Consultations
- Follow-Up Care
- Show All
- Medication
- Medication Summary
- Penicillins, Natural
- Penicillins, Amino
- Cephalosporins, First Generation
- Cephalosporins, Second Generation
- Cephalosporins, Third Generation
- Macrolides
- Analgesics, Other
- NSAIDs
- Anticholinergics, Respiratory
- Antihistamines, First Generation
- Antitussives, Non-Narcotic Combos
- Antitussives, Opioid Analgesics
- Alpha/Beta-Adrenergic Agonists
- Corticosteroids
- Decongestants, Systemic
- Decongestants, Intranasal
- Show All
- Questions & Answers
- Media Gallery
- Tables
- References




