Practice Essentials
Renal artery stenosis (RAS) is the major cause of renovascular hypertension and may account for 1-10% of the 50 million cases of hypertension in the United States population. [1] See the image below.
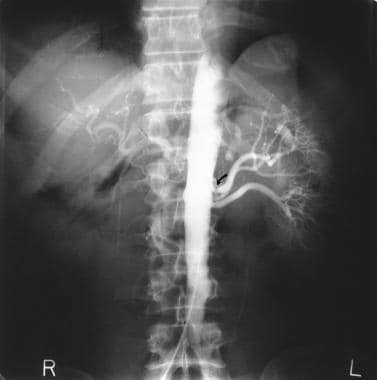 Renal artery stenosis/renovascular hypertension. Flush aortogram in a 32-year-old man with familial hypercholesterolemia and difficult-to-control hypertension. Radiograph shows a complete occlusion of the right renal artery and marked stenosis of the left renal artery (arrow).
Renal artery stenosis/renovascular hypertension. Flush aortogram in a 32-year-old man with familial hypercholesterolemia and difficult-to-control hypertension. Radiograph shows a complete occlusion of the right renal artery and marked stenosis of the left renal artery (arrow).
Apart from its role in the pathogenesis of hypertension, renal artery stenosis is also being increasingly recognized as an important cause of chronic kidney insufficiency and end-stage kidney disease. In older individuals, atherosclerosis is by far the most common etiology of renal artery stenosis. [2, 3] Fibromuscular dysplasia may also cause renal artery stenosis, especially in females younger than 50 years. [4] As the renal artery lumen progressively narrows, kidney blood flow decreases. Eventually, the decreased perfusion compromises kidney function and structure.
Patients with renal artery stenosis may present with one or more of the following (see Presentation):
-
Abdominal bruit
-
Azotemia
-
Sudden worsening of hypertension or kidney function
-
Acute kidney injury or decreased kidney function after initiation of antihypertensive therapy, especially with angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs) [5]
-
Unexplained kidney insufficiency, in elderly patients
-
Congestive heart failure, with poor control of hypertension and kidney insufficiency in the absence of a significant decrease in ejection fraction (so-called flash pulmonary edema) [6]
The workup in a patient with possible renal artery stenosis includes laboratory studies of kidney function and imaging studies of the kidneys and renal circulation (see Workup). Treatment includes pharmacologic control of hypertension and serum cholesterol levels, with surgical or percutaneous revascularization a consideration in selected patients (see Treatment and Medication). [7, 8] Guidelines covering the diagnosis and medical and surgical therapy of renal artery stenosis have been published (see Guidelines).
For patient education information, see Renal Artery Stenosis.
Pathophysiology
In patients with atherosclerosis, the initiator of endothelial injury is not clear. However, dyslipidemia, hypertension, cigarette smoking, diabetes mellitus, viral infection, immune injury, and increased homocysteine levels may contribute to endothelial injury.
The formation of atherosclerotic lesions involves increased permeability of endothelium to plasma macromolecules (eg, low-density lipoprotein [LDL]), increased turnover of endothelial cells and smooth muscle cells, and increased numbers of intimal macrophages. When atherogenic lipoproteins exceed certain critical levels, the mechanical forces may enhance lipoprotein insudation in these regions, leading to early atheromatous lesions.
Renal blood flow is 3- to 5-fold greater than the perfusion to other organs because it drives glomerular capillary filtration. Both glomerular capillary hydrostatic pressure and renal blood flow are important determinants of the glomerular filtration rate (GFR). [9]
In patients with renal artery stenosis, the chronic ischemia produced by the obstruction of renal blood flow leads to adaptive changes in the kidney that are more pronounced in the tubular tissue. These changes include atrophy with the following:
-
Decreased tubular cell size
-
Patchy inflammation and fibrosis
-
Tubulosclerosis
-
Atrophy of the glomerular capillary tuft
-
Thickening and duplication of the Bowman capsule
-
Intrarenal arterial medial thickening
In patients with renal artery stenosis, the GFR is dependent on angiotensin II and other modulators that maintain the autoregulation system between the afferent and efferent arteries and can fail to maintain the GFR when renal perfusion pressure drops below 70-85 mm Hg. Significant functional impairment of autoregulation, leading to a decrease in the GFR, is not likely to be observed until arterial luminal narrowing exceeds 50%.
The degree of renal artery stenosis that would justify any attempt at either surgical intervention or radiologic intervention is not known. One study found that when the pressure distal to renal artery stenosis was less than 90% of aortic pressure, renin release from the affected kidney was significantly elevated (renin being measured in the ipsilateral renal vein). This might be useful as a functional measurement of significant renovascular stenosis leading to hypertension and, thus, a marker of greater likelihood of benefit from angioplasty and stenting. [10, 11]
Etiology
Risk factors associated with ischemic renal disease (IRD) are as follows:
-
Hypertension: Of patients with IRD, 35% can be normotensive
-
Advanced age: Numerous cases occur in persons aged 60-69 years; incidence increases in persons older than 70 years
-
Kidney insufficiency
-
Extrarenal atherosclerosis
-
Diabetes mellitus
-
Smoking
In young adults, fibromuscular dysplasia is a common cause of bilateral renal artery stenosis. [5]
Epidemiology
In patients with mild hypertension, the prevalence of renal artery stenosis is probably less than 1%, while in those with acute as high as 10 % to 40% in patients with acute, severe, or refractory hypertension, the prevalence may be as high as 10-40%. [12] Studies suggest that ischemic nephropathy may be responsible for 5-22% of advanced kidney disease in all patients older than 50 years.
A review of a random sample of Medicare claims data (patients 67 years of age and older) found that the incidence of atherosclerotic renovascular disease was 3.7 per 1000 patient-years. The prevalence decreased with advancing age; the adjusted odds ratio (OR) was 0.86 for patients age 75 to 84 years and 0.44 for those age ≥85 years, compared with those age 67 to 74 years. The prevalence was highest in whites (adjusted OR for Blacks, 0.66). [13]
RVD is less common in blacks than in whites. The incidence rate in two studies of patients with severe hypertension was 27-45% in whites versus 8-19% in blacks. [14]
Although the incidence of atherosclerotic RVD is independent of sex, Crowley et al showed that female sex (as well as older age, elevated serum creatinine level, coronary artery disease, peripheral vascular disease, hypertension, and cerebrovascular disease) is an independent predictor of RVD progression. [15]
In 1964, Holley et al reported data from 295 consecutive autopsies performed in their institution during a 10-month period. [16] The mean age at death was 61 years. The prevalence rate of renal artery stenosis was 27% of 256 cases identified as having history of hypertension, while 56% showed significant stenosis (>50% luminal narrowing). In normotensive patients, 17% had severe renal artery stenosis (> 80% luminal narrowing). In those older than 70 years, 62% had severe renal artery stenosis.
Another similar autopsy study reported similar results, with 5% of patients older than 64 years showing severe stenosis; this figure increased to 18% for patients aged 65-74 years and 42% for patients older than 75 years.
Renal artery stenosis develops in 1%-12% of transplanted kidneys and is the principal vascular complication of kidney transplantation. [17, 18] Risk factors include older age in donors and recipients and expanded donor criteria. These cases most often occur 3-6 months after kidney transplantation. [17]
Prognosis
The consequences of renal artery stenosis are hypertension, which may be particularly difficult to control or may require multiple antihypertensive agents (with increased adverse effects), and progressive loss of renal function (ischemic nephropathy).
In addition, the discovery of atherosclerotic renal vascular disease (RVD) frequently occurs in the setting of generalized vascular disease (ie, cerebral, cardiac, peripheral), with the co-morbidity associated with disease in those vascular beds. Thus, any therapeutic intervention for renal artery stenosis should logically take into account the underlying prognosis associated with these co-morbidities.
Researchers have studied the natural history of atherosclerotic renal artery stenosis by obtaining images from sequential abdominal aortographs or duplex ultrasound scans in patients with documented renal artery lesions who have been treated medically. Most studies show that progressive arterial obstruction occurs in 42-53% of patients with atherosclerotic renal artery stenosis, often within the first 2 years of radiographic follow-up. The incidence rate of progression to complete renal artery occlusion in these studies ranges from 9-16%; this often occurs in patients with a high-degree stenosis. In a study of 85 patients at the Cleveland Clinic who were followed for 3-172 months, patients with mild-to-moderate stenosis remained unchanged upon follow-up, and 39% of patients with greater than 75% lesions progressed to total occlusion. [19]
-
Renal artery stenosis/renovascular hypertension. Left, Sonograms of the kidneys on a 57-year-old woman with difficult-to-control hypertension shows kidneys of uneven sizes: The left kidney is 96 mm, and the right kidney is 63 mm. Top right, Isotopic renogram (obtained with technetium mercaptoacetyltriglycine [MAG3]) after captopril shows a markedly depressed renal function in the right kidney. Bottom right, Analogous images show negligible activity in the right kidney. Note that this pattern is more typical for DTPA than MAG3 (as DTPA depends on the glomerular filtration rate for uptake which is decreased after captopril in renovascular hypertension [RVHT]). In severe cases of RVHT, MAG3 uptake can be decreased, as in this case. However, typically, uptake is preserved with decreased cortical excretion.
-
Renal artery stenosis/renovascular hypertension. Left, Flush aortogram in a 63-year-old man with hypertension shows marked stenosis of the right renal artery and complete occlusion of the left renal artery. Note the extensive atheroma in the aorta and iliac arteries. Right, nephrogram-phase image shows a significantly smaller left kidney with a faint nephrogram. Some blood supply to the left kidney is retained via collaterals (see image on the left).
-
Renal artery stenosis/renovascular hypertension. Flush aortogram in a 32-year-old man with familial hypercholesterolemia and difficult-to-control hypertension. Radiograph shows a complete occlusion of the right renal artery and marked stenosis of the left renal artery (arrow).
-
Three-dimensional gadolinium-enhanced magnetic resonance angiograms (MRAs) show medial fibroplasia, which appears as classic string-of-beads sign. This sign is due to multiple stenoses with intervening outpouchings that form a chain. In this case, the lesions involve the main right renal artery and the right accessory renal artery in a 37-year-old man with difficult-to-control hypertension.
-
Conventional flush aortogram in a 47-year-old woman with difficult-to-control hypertension shows the characteristic string-of-beads sign (arrows) of the right renal artery due to medial fibroplasia.








