Overview
Pneumonia is the leading infectious cause of death in developed countries. [1, 2] Among the vast diversity of respiratory pathogens, fungi account for only a small portion of community-acquired and nosocomial pneumonias. However, fungal respiratory infections generate concern in the expanding population of immunosuppressed patients. [1] Fungi may colonize body sites without producing disease or they may be a true pathogen, generating a broad variety of clinical syndromes. [3]
Fungal pneumonia is an infectious process in the lungs caused by one or more endemic or opportunistic fungi. Fungal infection occurs following the inhalation of spores, after the inhalation of conidia, or by the reactivation of a latent infection. Hematogenous dissemination frequently occurs, especially in an immunocompromised host.
Endemic fungal pathogens (eg, Histoplasma capsulatum, Coccidioides immitis, Blastomyces dermatitidis, Paracoccidioides brasiliensis, Sporothrix schenckii, Cryptococcus neoformans) cause infection in healthy hosts and in immunocompromised persons, in defined geographic locations of the Americas and around the world.
Opportunistic fungal organisms (eg, Candida species, Aspergillus species, Mucor species) tend to cause pneumonia in patients with congenital or acquired defects in the host immune defenses. Hyalohyphomycosis is a broad term that describes infections due to a number of rare and emerging heterogeneous fungi that when isolated from infected lung tissue, appear as hyaline (lightly colored), filamentous fungi difficult to distinguish from Aspergillus. These genera include Scedosporium, Fusarium, Paecilomyces, Acremonium, and Trichoderma and are described in more detail in the article "Rare and Emerging Fungal Pulmonary Infections".
The diagnosis of fungal pneumonias is difficult to prove and is often made on a presumptive basis. It relies on a combination of clinical, radiologic, and microbiological factors. [4] Candida organisms and some ubiquitous filamentous fungi (Aspergillus and Scedosporium) can be isolated from oropharyngeal and respiratory tracts as colonizers without evidence of invasion or symptoms until a breakdown of tissue barriers or of the host's immune system occurs. Nonmolecular fungal markers in serum or other biological samples represent a noninvasive diagnostic tool, which can help in therapeutic decisions. [1]
The individual prognosis is often linked to the severity and outcome of the underlying disease and to whether a reversal of factors affecting the patient's immune status is possible.
Pulmonary nodules resulting from fungal infection are seen below.
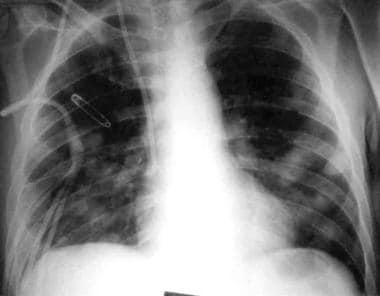 Chest radiograph showing multiple pulmonary nodules. The patient was treated with corticosteroids for acute graft versus host disease following bone marrow transplantation for chronic myeloid leukemia. The patient smoked marijuana for 2 weeks prior to this chest radiograph being taken. Bronchoalveolar lavage revealed Aspergillus niger and other species on fungal cultures.
Chest radiograph showing multiple pulmonary nodules. The patient was treated with corticosteroids for acute graft versus host disease following bone marrow transplantation for chronic myeloid leukemia. The patient smoked marijuana for 2 weeks prior to this chest radiograph being taken. Bronchoalveolar lavage revealed Aspergillus niger and other species on fungal cultures.
Complications of fungal pneumonia
Complications of fungal pneumonia include (1) disease dissemination to other sites (ie, brain, meninges, skin, liver, spleen, kidneys, adrenals, heart, eyes) and sepsis syndrome and (2) blood vessel invasion, which can lead to hemoptysis, pulmonary infarction, myocardial infarction, cerebral septic emboli, cerebral infarction, or blindness.
Other complications may include the following:
-
Bronchopleural or tracheoesophageal fistulas
-
Chronic pulmonary symptoms
-
Mediastinal fibromatosis (histoplasmosis)
-
Broncholithiasis (histoplasmosis)
-
Pericarditis and other rheumatologic symptoms
Treatment of fungal infection
Therapy for fungal pneumonias must include antifungal agents. The type of antifungal drug employed must be selected based on the particular pathogen that is isolated or that is clinically suspected. Many classes of antifungal agents are now available, including the classic antibiotics; first-, second-, and third-generation triazoles; and the echinocandins. Amphotericin B is less frequently used and, when used, is often given as a liposomal formulation to decrease toxicity. [5]
Risk Factors
Workers or farmers with heavy exposure to bird, bat, or rodent droppings or other animal excreta in endemic areas are predisposed to any of the endemic fungal pneumonias, such as histoplasmosis, in which the environmental exposure to avian or bat feces encourages the growth of the organism. In addition, farmers, nursery workers, landscapers, and gardeners are at higher risk of acquiring sporotrichosis because of their chance of cuts or puncture wounds while working with soil.The Pseudoallescheria boydii/Scedosporium apiospermum complex has been implicated as an important pathogen in delayed disseminated infections among victims of near-drowning in polluted waters [6] or recent natural disasters such as the Indonesian tsunami in 2004. [7]
Coccidioides species are dimorphic existing as mold in the environments and as spherules in vivo. Arthroconidia in mold state are easily dispersed and inhaled into the lungs. [5] Therefore, because of its high virulence, it is also a threat among laboratory personnel working with this fungus. [5]
Conditions that predispose patients to any of the opportunistic fungal pathogens are as follows:
-
Acute leukemia or lymphoma during myeloablative chemotherapy
-
Bone marrow or peripheral blood stem cell transplantation
-
Solid organ transplantation on immunosuppressive treatment
-
Prolonged corticosteroid therapy
-
Acquired immunodeficiency syndrome
-
Prolonged neutropenia from various causes
-
Congenital immune deficiency syndromes
-
Postsplenectomy state
-
Genetic predisposition
With regard to predisposition through stem cell transplants, certain toll-like receptor (TLR) polymorphisms (eg, TLR 4 haplotype S4) in an unrelated stem cell donor can increase the risk of invasive aspergillosis in the transplant recipient. [8] Similarly, TLR1 and TLR6 polymorphisms in the recipient have been associated with susceptibility to invasive aspergillosis after allogeneic stem cell transplantation. [9]
Epidemiology of Fungal Pneumonia
Distribution endemic fungi in the United States
Endemic fungi are prevalent in the Mississippi River Valley and the Ohio River Valley (eg, H capsulatum, B dermatitidis), the southwestern United States, and northwestern Mexico (eg, C immitis).
The environmental niche for H capsulatum is soil enriched by nitrogen contained in birds' and bats' droppings, [5] whereas B dermatitidis is found in the soil and decaying wood, especially in waterways. [5]
Coccidioides species is found in alkaline, highly salinic, sandy soils and extreme temperatures.
Sporotrichosis has been described worldwide; prevalence is higher in tropical and temperate zones. Infection generally occurs following traumatic inoculation with soil, plants, and organic matter contaminated with the fungus. However, it occasionally may be inhaled, causing pneumonitis that often cavitates. [10]
International distribution and incidence of fungal infection
These fungi have caused several pneumonia outbreaks in Argentina and other areas of Central and South America. P brasiliensis is restricted to Central and South America. African histoplasmosis, which is caused by H capsulatum duboisii, is limited to equatorial Africa between 20° N and 10° S, which includes Gabon, Uganda, and Kenya.
The other opportunistic organisms are ubiquitous, are usually found worldwide, and tend to cause disease in hosts with abnormal immune defenses. For instance, C neoformans can affect people with intact immune systems at a rate of 0.2 cases per million population per year. Prior to the advent of highly active antiretroviral therapy (HAART), approximately 80-90% of patients with acquired immunodeficiency syndrome (AIDS) developed cryptococcosis. [11]
Morbidity and mortality in fungal infection and pneumonia
The endemic fungal pneumonias are generally self-limited in healthy hosts. C immitis is the most virulent, yet 90% of patients recover without treatment. However, patients with fungal pneumonias may develop chronic pulmonary complications (eg, cavitation, pleural effusions, bronchopleural fistulas) or extrapulmonary complications. In patients with AIDS, the mortality rate is as high as 70%.
Aspergillosis represents the leading cause of invasive pulmonary lung infection and death among patients who are neutropenic (from either leukemia chemotherapy or bone marrow transplantation) with a mortality rate of 50-85%. More often, in the case of aspergillosis and candidal infections or meningoencephalitis in the case of cryptococcosis, the cause of mortality in patients who are immunocompromised is disseminated fungal disease. [12]
Mucormycosis represents the second most common cause of fungal pneumonia, accounting for approximately 10% of all invasive pulmonary infections in immunosuppressed patients and resulting in significant morbidity and mortality. Patients with hematologic malignancies are at highest risk, but uncontrolled diabetes mellitus and iron overload are important predisposing factors. [1] Rhizopus, Mucor, Absidia (Lichtheimia), and Rhizomucor species are the most commonly implicated. [1, 5]
P boydii or its asexual form, S apiospermum, is now considered an emerging pathogen causing pneumonia and disseminated infections in the same immunocompromised hosts as aspergillosis. Scedosporium species (including prolificans) are inherently resistant to amphotericin B and echinocandins, and infections carry high mortality rates, especially in the persistently profound neutropenic patient. [13]
The mortality rate for untreated disseminated histoplasmosis is 80%, but, with treatment, the rate is reduced to 25%.
Candida albicans and Candida glabrata are ubiquitous commensals of humans and can be found especially in the oral cavity and gastrointestinal tract of most healthy humans. On the other hand, they are also the most pathogenic yeasts. [14] Among the Candida species, C albicans and C glabrata rank as the two most frequently isolated organisms. [14] Despite the frequent isolation of Candida species from respiratory samples in nonneutropenic patients, the organisms are not considered causes of pneumonia regardless of the species isolated. [15] Pneumonia from Candida species is exceptional in nonneutropenic patients. [15]
Sporothrix schenckii is the etiological agent of sporotrichosis, a chronic fungal infection that most frequently affects cutaneous and subcutaneous tissues and adjacent lymphatics. [10] However, extracutaneous forms have been described with no history of traumatic injuries, making the diagnosis difficult. [10] Pulmonary presentation is rare and may be caused by the dymorphic fungus S schenckii and even more rarely by other Sporothrix species. Lately, recognition of this condition has increased as more cases have been reported. [16] In immunocompromised patients, disseminated sporotrichosis may be associated with significant morbidity and, possibly, mortality.
Race-associated characteristics
Although no race predilection is described, C immitis causes more severe disease in patients of African American [5] or Philippine descent.
Sex predilection
Endemic fungal disease affects men (75-95%) more often than women. Estrogen-mediated inhibition of mycelium-to-yeast transformation may be responsible for the male predominance. Estrogen also seems to have a protective effect against cryptococcal infection. Cryptococcosis has a male-to-female ratio of 2-3:1.
Effects of Disseminated Fungal Disease
Fungi may simply colonize body sites with no apparent disease, or they may invade, producing a wide variety of syndromes. The development of disease is a result of the susceptibility of the host and the virulence of the pathogen. [1]
Endemic mycoses with associated dissemination can affect skin (eg, papules, pustules, plaques, ulcers, abscesses, proliferative lesions that may mimic skin cancer as in B dermatitidis infection), bone and joints, and the brain and meninges (meningitis with poor prognosis [10-20%], brain abscess in infection with Aspergillus and Mucor species).
Other affected sites include the following:
-
Kidneys
-
Liver and spleen (hepatosplenic candidiasis)
-
Muscle (Candida species)
-
Eye (endophthalmitis; in Candida species infection)
-
Nasal passages and sinuses (Aspergillus and Mucor species)
-
Bloodstream and bone marrow (septicemia or sepsis syndrome)
Patient History
History findings in persons with fungal pneumonia may include the following:
-
Fever
-
Cough, usually nonproductive
-
Pleuritic chest pain or dull discomfort
-
Progressive dyspnea leading to respiratory failure
-
Airway obstructive symptoms from enlarged mediastinal adenopathy in the endemic mycoses
-
Hemoptysis (in invasive aspergillosis or mucormycosis)
-
History of travel to or exposure in areas containing endemic mycoses
-
Symptoms from involvement of extrapulmonary systems (may suggest disease)
-
Rheumatologic syndromes (common among endemic mycoses) - Arthritis and arthralgia, erythema nodosum, erythema multiforme, and pericarditis
-
Endemic mycoses with associated dissemination
-
Hypersensitivity or allergic reactions
-
Extrapulmonary sites in individuals who are immunocompromised
-
Meningoencephalitis in patients with AIDS and cryptococcosis
In individuals who are neutropenic or immunocompromised, persistent fever (even before pulmonary findings) may be an early sign of infection, especially if the fever is unresponsive to broad-spectrum antibiotics.
Hypersensitivity or allergic reactions include allergic bronchial asthma (Aspergillus species, Candida species), allergic bronchopulmonary mycoses (Aspergillus species, Candida species), bronchocentric granulomatosis (necrotizing granulomatous replacement and eosinophilic infiltration of bronchial mucosa in infection with Aspergillus species), and extrinsic allergic alveolitis (malt worker's lung, farmer's lung).
Physical Examination
Signs and symptoms of fungal pneumonia are not specific, and are indistinguishable from those associated with respiratory infections of other origins.
Physical examination findings in patients with fungal pneumonia may include the following:
-
Temperature elevation
-
Tachycardia
-
Tachypnea
-
Respiratory distress
-
Rales
-
Signs of pulmonary consolidation
-
Pleural rub
Important possible extrapulmonary findings include the following:
-
Meningitis (neck stiffness, headaches, mental status change)
-
Brain abscesses
-
Skin lesions (pustules, papules, plaques, nodules, ulcers, abscesses, hemorrhagic lesions, mycetomas)
-
Rheumatologic and allergic findings
-
Pericardial rub
Differentials in Fungal Pneumonia
Conditions that can mimic the symptoms of fungal pneumonia include the following:
-
Eosinophilic pneumonia
Workup Considerations
The mortality due to fungal respiratory infections among immunosuppressed populations has remained elevated despite the arrival of new antifungal medications. The paucity of specific signs of infections and the low sensitivity of conventional culture-based methods for its diagnosis results in delayed initiation of antifungal therapy. [1]
Nonculture-based diagnostic tools, such as galactomannan (GM) and beta-D-glucan (BG), are part of the diagnostic workup of invasive fungal pneumonia with other clinical, radiologic, and microbiologic criteria.
A retrospective multicenter study from France during the first wave of the coronavirus disease 2019 (COVID-19) pandemic recommends that for diagnosing COVID-19–associated pulmonary aspergillosis, examination of respiratory specimens is the best approach because serum biomarkers are rarely positive. [17]
CBC Count With Differential
The total white blood cell (WBC) count may be elevated in normal hosts with endemic mycoses.
Eosinophilia can be observed in the differentials, particularly in persons with coccidioidomycosis.
If the patient presents with neutropenia or leukopenia, the possibility of an opportunistic infection with Candida, Aspergillus, Mucor, or Scedosporium organisms is increased.
Sputum Examination and Potassium Hydroxide Stain
This study may show fungal hyphae or yeasts. However, the results must correlate with the clinical situation, because saprophytic colonization occurs in the oropharyngeal or respiratory tract of some patients and may not necessarily indicate invasive infection.
Carefully transport, process, and culture specimens that may be contaminated by bacteria, may be saprophytic yeasts endogenous to the oral cavity, and may be airborne conidia of saprophytic fungi.
The diagnosis of pulmonary cryptococcal infection is confirmed if the organism is grown in culture from sputum or BAL fluid in a patient who has clinical symptoms and radiographic finding compatible with cryptococcosis. [5]
Histoplasmosis is definitively diagnosed by growth of the organism in sputum; BAL fluid, lung tissue, or mediastinal nodes can be cultured. [5]
In pulmonary sporotrichosis, the recovery of the fungi by culture of sputum and/or positive bronchoscopy are required for diagnosis. [16]
Cultures from sputum samples collected by fiber optic bronchoscopy are not valuable for the diagnosis of pneumonia by Candida. [15] To make the diagnosis, a biopsy is required to demonstrate tissue invasion. Colonization of the respiratory tract by Candida is very frequent in critically ill patients with mechanical ventilation, but pneumonia by Candida is extremely rare because the innate defense mechanisms of the lungs make them relatively resistant to candida invasion. [15]
Scedosporium species tend to grow well on routine fungal media, but, when dealing with BAL fluid or tenacious respiratory secretions, selective media (cycloheximide or benomyl agar) are recommended for their isolation. [13]
Blood and Urine Cultures
Obtain a blood culture to identify Candida species (lysis centrifugation) or B dermatitidis if the patient has disseminated disease.
Obtain a urine fungal culture in men after a prostatic massage, to identify Cryptococcus or Blastomycosis species.
Nonculture Methods for Detecting Fungal Infections
These provide a more rapid and sensitive test when compared with culture methodology. Various antigen detection assays, such as galactomannan enzyme immunoassay for detection of invasive aspergillosis, are now in clinical use. Polymerase chain reaction (PCR)–based assays are also available for detecting various pathogens, including Aspergillus, Histoplasma, and Candida species. [18, 19, 20]
Comparison of these assays (antigen detection using enzyme-linked immunosorbent assay [ELISA] or latex agglutination and molecular detection with PCR) show equal specificities for all 3 assays (≥97%) in the detection of Candida species. PCR-based assays are most sensitive compared with ELISA and latex agglutination (95%, 75%, and 25%, respectively).
The newest available testing in the diagnosis of blastomycosis is an enzyme immunoassay performed on urine or serum that detects a cell wall galactomannan antigen found in B dermatitidis. However, the cross reactivity with H capsulatum is close to 100%. [5] Therefore, in patients with blastomycosis, the sensitivity or specificity of these tests is not clear. [5]
For Aspergillus species antigen, galactomannan assay findings may be positive in the blood very early prior to clinical suspicion of invasive fungal infection and may be of use in monitoring and preemptive treatment in high-risk populations. [1, 21, 22, 23]
Using a galactomannan platelia Aspergillus enzyme immunoassay approved by the US Food and Drug Administration (FDA), investigators showed that two consecutive samples with an optical index of 0.5 provided the highest test accuracy (specificity, 97.5%; sensitivity, 92.1%; positive predictive value, 87.5%; negative predictive value, 98.5%). [24] Testing in bronchoalveolar lavage (BAL) fluid increased the sensitivity compared with serum galactomannan assay from 71-100%. [25] Care should be taken, however, because false-positive results have been reported in patients taking piperacillin-tazobactam antibiotics and certain intravenous fluids, such as plasmalyte. [26]
Beta-glucan testing is also available and may be comparable or more sensitive than galactomannan assays in diagnosing invasive aspergillosis and can detect a broad spectrum of invasive fungal pathogens, including Pneumocystis jirovecii. [1, 27, 28] Several kits are available worldwide. False-positive results have also been reported in patients receiving fungal-derived antibiotics and cross-reactions have been reported with Pseudomonas aeruginosa infections. [29]
The molds causing mucormycosis, which belong to the subphylum Mucoromycotina, do not contain galactomannan or beta-glucan in their cell wall. Therefore, mucormycosis cannot be diagnosed with the galactomannan or beta-glucan assays. [1]
Aspergillus PCR is most sensitive (100%) when performed on the bronchial lavage fluid of patients with invasive pulmonary aspergillosis, but it is only 40-66% sensitive when performed on the blood. No standardized protocols have been established among laboratories performing this assay. [12, 19, 29]
ELISA or latex agglutination is 70-80% sensitive for identifying H capsulatum and C immitis. PCR for H capsulatum from the bronchoalveolar lavage fluid aids in the rapid detection within 24 hours in a patient with AIDS, and this has been confirmed 10 days later based on the growth and culture isolation of the organism from various tissues.
Serology
The utility of serology depends on the individual fungal infectious agent. Antibody detection for the identification of C immitis is highly useful for all forms of pulmonary infection caused by this fungi. [5] Serology also plays an important role in the diagnosis of acute pulmonary and chronic cavitary pulmonary histoplasmosis. Both complement fixation and immunodiffusion tests should be ordered, [5] but these tests are of less utility if the pulmonary infection is due to other fungi.
Serology testing for blastomycosis provides little clinical diagnostic help because of the insensitivity of testing for this fungus and the antibody cross-reactivity that occurs with other fungal infections.
Patients with pulmonary sporotrichosis will have antibody against S schenckii; however, it is highly variable in sensitivity and specificity. Thus, it may not be useful in the diagnosis of the disease.
Detection of the polysaccharide capsule antigen in serum plays an important role in the diagnosis of disseminated cryptococcosis, but its sensitivity decreases in those patients not infected with human immunodeficiency virus, and also disease limited to the lung. [1]
Chest Radiography
Patchy infiltrate, nodules (seen in the image below), consolidation, cavitation, or pleural effusion may be observed.
Mediastinal adenopathy is common in patients with endemic fungal pneumonias. The adenopathy may be either unilateral or bilateral.
In neutropenic patients infected with aspergillosis (60%), pulmonary nodules surrounded by ground-glass opacity called “halo sign” [1, 5] is a common finding. On the other hand, lung transplant recipients present less specific patchy infiltrates. [5]
Miliary infiltration occurs in patients with disseminated disease.
Chest radiograph showing multiple pulmonary nodules. The patient was treated with corticosteroids for acute graft versus host disease following bone marrow transplantation for chronic myeloid leukemia. The patient smoked marijuana for 2 weeks prior to this chest radiograph being taken. Bronchoalveolar lavage revealed Aspergillus niger and other species on fungal cultures.
CT Scanning and MRI
Chest CT scanning
This imaging study plays a role in the early diagnosis of nonspecific infiltrates in patients who are immunocompromised. [30]
High-resolution chest computed tomography (CT) scanning allows observation of the halo sign in patients with aspergillosis. This is a nodular lesion usually surrounded by a ground-glass opacity or halo. As many as 61% of 235 patients with invasive aspergillosis were found to have the halo sign in one study. [31] Lung lesions from aspergillosis are shown below.
Obtaining a CT scan of the abdomen and brain may reveal sites of dissemination.
 CT scan of a patient with invasive aspergillosis showing multiple lung lesions. The cavitary lesion on the left lung shows a ground-glass halo sign.
CT scan of a patient with invasive aspergillosis showing multiple lung lesions. The cavitary lesion on the left lung shows a ground-glass halo sign.
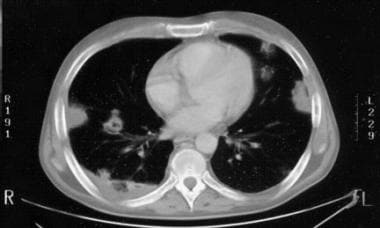 CT scan of aspergillosis of the lungs showing multiple pleural-based and lung parenchymal lesions.
CT scan of aspergillosis of the lungs showing multiple pleural-based and lung parenchymal lesions.
CT scans should be obtained at the first hint of pulmonary infection in patients at risk of mucormycosis because of the high mortality in this patient population. In patients with hematological malignancies, several nonspecific findings have been proposed to differentiate mucormycosis from other infections, especially aspergillosis. These include the presence of multiple nodules and pleural effusions and the development of a “reversed halo,” which is a ground-glass attenuation in the center of a nodule with a surrounding zone of consolidation. [5, 32] The reversed halo sign is not exclusive to mucormycosis; it might also be found in patients with paracoccidioidomycosis, histoplasmosis, cryptococcosis, [32] and even nonfungal causes like tuberculosis and sarcoidosis. [33] In the setting of severe neutropenia however, it warrants a high suspicion for pulmonary mucormycoses [34] and initiation of appropriate empiric treatment while awaiting culture results.
MRI of lung lesions
Magnetic resonance imaging (MRI) may reveal the hemorrhagic content of Aspergillus lesions.
Procedures
Fiberoptic bronchoscopy (procedure of choice) is used to obtain bronchial lavage specimens for staining and culture techniques and transbronchial biopsy specimens for identification of fungal tissue invasion. This procedure reveals positive results in 75-90% of endemic mycoses, shows a 50-90% yield in cryptococcal disease, and shows varying yields in Aspergillus and Candida infections, for which clinical correlation is still important.
The yield of isolating Aspergillus from bronchoalveolar lavage specimens may also depend upon the underlying condition and the leukocyte count of the patient. One study demonstrated that there was little value in doing bronchoscopy and bronchoalveolar lavage in acute leukemia patients with leukocyte counts of less than 100/µL compared with nonleukemia patients such as allogeneic hematopoietic stem cell recipients. [35]
Transthoracic CT-guided fine-needle aspiration of pulmonary nodules can provide material for histopathology and for special staining techniques and culture. Obtaining specimens in this manner might allow for avoidance of an open lung biopsy.
Occasionally, performing an open lung biopsy is the only way to prove invasive disease for Aspergillus or Candida organisms. However, this procedure may be difficult to perform in patients with severe neutropenia and thrombocytopenia who are in respiratory failure.
Perform a lumbar spinal puncture in patients with suspected cryptococcosis or disseminated disease with central nervous system (CNS) symptomatology in order to detect the polysaccharide capsule antigen by latex agglutination or enzyme immunoassay.
Conduct a bone marrow aspiration and biopsy if the patient has persistent fever or suspected disseminated disease or if the patient has hematologic findings, such as thrombocytopenia or neutropenia.
Histologic Findings
Biopsy specimens show the following:
-
Caseating or necrotizing granulomas with intracellular organisms inside macrophages (eg, H capsulatum, C immitis)
-
Fungal hyphae in infection with Aspergillus, Mucor, or Scedosporium species
-
Intracellular yeast organisms in Candida species infections
Histopathology
Histopathology findings are as follows:
-
Aspergillosis: Nonpigmented (hyaline), septate hyphae with acute angle branching, but not specific
-
Mucormycosis: Nonpigmented (hyaline), broad non-septate hyphae presumptive evidence for mucormycosis
-
Cryptococcosis; Yeast forms with clear surrounding area are suggestive; mucicarmine stain is specific
-
Blastomycosis: Broad based budding yeast (10-15 µm); forms provide presumptive evidence of infection
-
Histoplasmosis: Small yeasts (2-4 µm) with narrow-based budding grouped in clusters inside macrophages; characteristic yeast forms provide presumptive evidence of infection
-
Coccidioidomycosis: Spherules large and specific, give presumptive diagnosis
-
Candidiasis: Small yeasts (3-5 µm) intermingled with pseudohyphae and/or hyphae; C glabrata does not produce filaments or pseudohyphae
-
Sporotrichosis: Dimorphic fungus, conidiophores, and conidia; cigar-shaped yeast may be visualized in tissue specimens stained with periodic acid-Schiff, Gomori methenamine-silver, or immunohistochemical stains
-
Scedosporium: Haphazardly branching hyphae and lemon-shaped conidia; parallel hyphae bridged at right angles producing letter-H patterns; purple conidia in tissue [36]
Treatment of Fungal Infection
In persons with endemic mycoses, spontaneous recovery usually occurs without treatment, especially in patients who are mildly affected and immunocompetent without dissemination; otherwise, administer treatment as outlined in the table below.
In cases in which aspergillosis, mucormycosis, and candidiasis occur in an immunocompromised host, reversing the factors affecting the patient's immune status is linked to successful recovery from the infection. Attempt ancillary interventions that may help to promote recovery from the opportunistic infection. These include (1) ensuring, with the use of growth factors, neutropenia recovery in patients receiving chemotherapy and bone marrow transplants; (2) withdrawing or tapering immunosuppressive drugs and steroids; and (3) removing infected or highly colonized catheters in patients with candidiasis.
Table. Medical and Surgical Fungal Therapy (Open Table in a new window)
Fungal Pathogen |
Indication for Antifungal Therapy |
Surgical Care and Other Treatments |
Antifungal Drugs Used |
Acute pulmonary histoplasmosis with hypoxia; prolonged moderate symptoms for more than 1 month; disseminated disease; immunosuppressed host Mortality rate for untreated disseminated disease at 80%; reduced to 25% with treatment |
Significant hemoptysis; recurrent pneumonia; repair of bronchopleural fistula Corticosteroids in severe hypoxia or ARDS Anti-inflammatory agents to treat rheumatologic syndromes |
Amphotericin B induces rapid response in patients who are severely ill or immunocompromised Azoles/triazoles in patients with milder illness |
|
Disseminated disease; chronic pulmonary disease; acute pulmonary infection with hypoxia or protracted morbidity (>1-2 mo); immunosuppressed host (worst outcome, 70% mortality) |
Surgical debridement or resection of infective tissue often necessary adjunct to antifungal treatment Anti-inflammatory agents for rheumatologic syndromes |
Amphotericin B effective in more than 90% of cases; first choice in severe cases or immunocompromised Fluconazole/itraconazole first choice in mild to moderate infection (or after improvement) Treatment less effective than in other endemic mycoses |
|
Persistent or recurrent symptoms of acute or chronic pulmonary disease or with pleural involvement; disseminated disease |
Steroids for ARDS |
Amphotericin B response rates of 77-90% of cases; for severe infection or immunocompromised Itraconazole successful in 90% of cases; for mild to moderate infection Ketoconazole response of 80%; poor outcome in patients who are immunosuppressed Fluconazole less effective, 65% response rate Chronic maintenance treatment essential for all patients with AIDS or meningitis |
|
Patients who are immunosuppressed and symptomatic; patients who are immunocompetent with disease progression; any patients with meningitis or disseminated disease |
N/A |
Amphotericin B in patients who are severely ill Fluconazole in milder cases or after clinical response to amphotericin B Lifelong maintenance therapy in AIDS patients may not be necessary as long as the patient's CD4 count is maintained above 100 cells/µL with HAART [37] Flucytosine may be of benefit when combined with amphotericin B in patients with severe or disseminated disease. [5] |
|
All patients with invasive disease; in patients who are immunosuppressed, early diagnosis and empiric treatment for persistent fever not responding to broad-spectrum antibiotics; high mortality once infiltrates and symptoms appear; prognosis ultimately linked to severity and outcome of underlying disease Mortality rate of 50-60% in patients with AIDS |
Rapid tapering of immunosuppressive agents and corticosteroids and reversal of neutropenia (if possible) |
Voriconazole is the new standard of care for invasive aspergillosis based on superiority over amphotericin B in primary therapy Lipid formulations of amphotericin B have at least equal efficacy but less toxicity compared with amphotericin B desoxycholate Oral voriconazole can be used to complete treatment with initial response to IV voriconazole or amphotericin B Posaconazole is second line agent Echinocandins second line agent when voriconazole is not tolerated or in combination with voriconazole in an attempt to enhance antifungal activity Isavuconazole has been shown to be not inferior to voriconazole for aspergillosis [38] |
|
Mortality rates as high as 70% in patients with invasive pulmonary mucormycosis |
Aggressive surgical debridement of necrotic tissue important in mucormycosis, especially if confined to lungs |
Lipid amphotericin B is the mainstay of therapy; posaconazol is poorly absorbed, considered second line Mucor species generally resistant to azoles (voriconazole has no activity against them) Echinocandins (Caspofungin) useful as salvage therapy Isavuconazole has been shown to be comparable to amphotericin B and posaconazole for mucormycosis [38] |
|
All patients with invasive disease or dissemination; important to reverse factors affecting immune status Expert recommendations and clinical practice guidelines do not recommend antifungal treatment facing isolation in respiratory samples regardless the number of positive samples [15] |
Rapid tapering of immunosuppressive agents and corticosteroids; important to remove indwelling infected intravenous lines or urinary catheters in setting of hematogenous spread |
Amphotericin B is mainstay Flucytosine may be of benefit when added to amphotericin B Fluconazole use in pulmonary disease not studied but is effective in hepatosplenic candidiasis and candidemia Echinocandins may be useful alternatives |
|
Management should be based in clinico-radiological manifestations; two presentations of pulmonary sporotrichosis: non-cavitary disease (multifocal) and cavitary disease (primary) [16] |
Surgical interventions when presence of cavitations and initial medical therapies have failed; used as adjunctive therapy |
Itraconazole as first line agent in mild to moderate cases Amphotericin B first line in life threatening conditions |
|
| Scedosporiosis | Emerging opportunistic pathogen in similar scenario as aspergillosis but highly resistant to amphotericin B and echinocandins; mortality rate is 54-78% in transplant recipients In near-drowning victims, close surveillance for clinical and radiographic findings with low threshold for empiric treatment |
Aggressive surgical debridement for disseminated disease in the form of subcutaneous abscesses, brain abscess, and others Granulocyte transfusions or growth factors to enhance neutrophil recovery |
Resistant to amphotericin B and echinocandins Voriconazole as single agent or in combination with other agents such as terbinafine [39] |
Pharmacologic treatment
When treatment is indicated, initiate antifungal agents as appropriate. Amphotericin B is the mainstay of initial therapy in many cases, especially for patients who are acutely ill. More expensive liposomal preparations of amphotericin B offer equal efficacy with less toxicity. In patients with invasive aspergillosis, including pulmonary aspergillosis, voriconazole is the new standard of care, based on its superiority over amphotericin B as primary therapy. [5, 12, 40, 41, 42] Vary the dose and treatment duration depending on the underlying pathogen causing the pneumonia.
Care should be taken regarding patients on long-term voriconazole treatment. Bone pain with radiologic evidence of periostitis and 10-fold increased fluoride levels have been reported in allogeneic stem cell transplant patients taking the drug for at least 3 months. Symptoms and findings were reversed with discontinuation of voriconazole. [43]
There is a possible association between the use of voriconazole in markedly immunosuppressed patients as prophylactic agent and the development of mucormycosis, but this matter is still controversial. [5]
Amphotericin B is available in a variety of formulations. Conventional amphotericin B injection contains amphotericin B and sodium deoxycholate as the solvent vehicle.
Amphotericin B cholesteryl sulfate complex (ABCD, Amphotec) consists of a 1:1 molar ratio of amphotericin B to cholesteryl sulfate in a colloidal dispersion, forming a bilayer in microscopic, disk-shaped particles that have a diameter of approximately 115 nm and a thickness of 4 nm.
Amphotericin B lipid complex (ABLC, Abelcet) is composed of amphotericin B and phospholipid complex, with a microscopic, ribbonlike structure having a diameter of approximately 2-11 µm.
Liposomal amphotericin B (L-AmB, AmBisome) contains amphotericin B intercalated in a unilamellar bilayer liposomal membrane; has a liposomal membrane diameter of less than 100 nm; and consists of hydrogenated soy phosphatidylcholine, cholesterol, distearoyl phosphatidylglycerol, and alpha tocopherol.
Some clinicians offer empiric therapy with conventional amphotericin B or liposomal amphotericin B for presumed fungal infections in patients who are febrile and neutropenic (eg, cancer, bone marrow transplantation, solid organ transplantation) and whose febrile state persists after receiving broad-spectrum antibiotics for a few days. Other agents that could be used in this setting are itraconazole and an echinocandin, namely, caspofungin. [44] The therapy is continued until the neutropenia resolves and the patient does not show a documented fungal infection or radiographic infiltrate.
Prophylactic therapy (suppressive therapy) with amphotericin B is used against recurrence or relapse of coccidioidomycosis, cryptococcosis, or histoplasmosis in individuals infected with the human immunodeficiency virus (HIV) who have received adequate treatment for the infection.
Other formulations, however, are starting to replace amphotericin B because of their ease of use (oral formulations) and lower toxicity for more long-term suppression. Posaconazole is used in the prophylaxis of invasive Aspergillus and Candida infections in severely immunocompromised patients receiving hematopoietic stem cell transplants who have graft versus host disease and in patients with hematologic malignancies who have chemotherapy-induced neutropenia. [45] While it used to be available only as an oral suspension given thrice daily, a delayed-release tablet formulation of posaconazole for once-daily administration allows for better bioavailability without being affected by food. The intravenous formulation is also administered once daily, but it has to be through a central line because of the presence of a solubilizing excipient SBECD (sulfobutylether-β-cyclodextrin), which can be potentially renal toxic and can accumulate in patients with moderate-to-severe renal failure. [46] Because of the large interindividual and intraindividual variations in bioavailability and drug-to-drug-interactions, therapeutic drug monitoring is recommended for posaconazole, especially if used in the therapeutic setting to treat invasive aspergillosis or zygomycosis.
Other antifungal agents used in the treatment of fungal pneumonia are fluconazole (Diflucan), itraconazole (Sporanox), flucytosine (Ancobon), and ketoconazole (Nizoral). Newer antifungal agents, such as the third-generation triazoles or the echinocandins, are more tolerable than amphotericin B or its liposomal preparations are and may even be more effective in first- or second-line treatment.
Isavuconazole has been approved by the FDA and the European Medicines Agency for the treatment of invasive aspergillosis and mucormycosis. Studies have shown it to be not inferior to voriconazole for aspergillosis and comparable to amphotericin B and posaconazole for mucormycosis. [38]
There have been increasing reports of azole resistance in Aspergillus species. This might be the result of the increasing use of these agents for prophylaxis and treatment of fungal infections; also there are associations with exposure to azole-like compounds used in the agricultural industry in some countries. In addition, some species have intrinsic resistance to various azoles. [5]
Caspofungin is approved for the treatment of invasive Aspergillus infections in patients unresponsive to or unable to receive amphotericin B. Combinations of a triazole with an echinocandin with or without amphotericin B have been anecdotally reported to be effective in some cases of resistant organisms, such as Mucor or Zygomycetes species. [44]
Echinocandins such as caspofungin, micafungin, and anidulafungin [47, 48, 49] offer a broad spectrum of activity for the many Candida species, including fluconazole-resistant strains. They also show effectiveness in Aspergillus infections alone or in combination with an azole.
Because of the introduction of these safer and (possibly) more potent agents, and owing to the ability to combine them together, the outlook for patients with invasive pulmonary infections, especially immunocompromised hosts, may be improving.
The role of combination therapy has been studied only in small retrospective studies with very unclear results. Combination therapy is usually not indicated in first-line treatment. In rare cases, it might be offered with a great deal of caution as second-line or salvage treatment. [39]
The establishment of neutrophil recovery or engraftment and the reduction of immunosuppression in certain patients who are at risk for fungal infections are likely to improve the chances of a successful treatment outcome. Granulocyte-macrophage colony-stimulating factor can theoretically augment pulmonary host defenses against A fumigatus infection.
Surgical care
Surgery may be indicated in invasive aspergillosis. [50] Surgery is indicated in patients with documented invasive aspergillosis who have been treated with antifungal agents but who have residual lesions. The surgery is performed to prevent disease relapse when additional immunosuppression is required. Surgery is also indicated as a means to prevent or treat massive bleeding, especially when the lung lesion is contiguous with a large blood vessel.
In cavitary pulmonary sporotrichosis, surgical management should be considered in the course of the disease, even for bilateral presentation, providing that the patient has adequate predicted respiratory reserves post-surgery, as delayed surgery may result in complications and poorer outcomes. [16]
Inpatient Considerations
Watch for rapidly progressive respiratory failure in patients who are neutropenic. Patients may require intubation and mechanical ventilatory support. In patients who are severely neutropenic, rapid progression of fungal pneumonia and dissemination of fungal infection (eg, aspergillosis, mucormycosis) necessitate a high degree of suspicion, early empiric antifungal therapy, and corrective measures (if possible) to reverse neutropenia or other causes of immunosuppression. [5]
Consider rapidly reducing or withdrawing immunosuppressive therapy (eg, corticosteroids), if feasible.
Correct hyperglycemia and acidosis.
Consider the correction of neutropenia via the administration of growth factors (eg, filgrastim [Neupogen], pegfilgrastim [Neulasta], sargramostim [Leukine]) or granulocyte transfusions.
Outpatient Considerations
Offer maintenance therapy to suppress disease reactivation or recurrent disease in patients infected with HIV or in other individuals who are immunocompromised.
Ensure appropriate follow-up care to monitor for possible recurrence.
Patients with ongoing immune deficiencies may require prolonged or lifelong maintenance therapy with triazole agents to prevent recurrences.
Clinical Consultations
A pulmonologist may perform diagnostic procedures (eg, bronchoscopy, bronchoalveolar lavage, transbronchial biopsy).
Interventional radiologists can perform needle aspirations, when necessary, for diagnosis.
Patients who are severely ill and progressively hypoxic may require intensive care, ventilatory support, and pressor support in the ICU under the care of a critical care intensivist.
Rheumatologists can assist with the rheumatologic syndromes manifesting with the endemic mycoses.
Infectious disease consultants may assist with the intricacies of antifungal treatment, especially with respect to the exact drugs, dose, duration, therapy length, maintenance treatment, and follow-up.
Deterrence and Prevention of Fungal Pneumonia
Instruct patients to avoid travel to and exposure in endemic areas.
Patients undergoing bone marrow transplantation or any period of prolonged neutropenia are advised to avoid activities (eg, gardening, cleaning, agitating debris) or objects (eg, potted plants, flowers, fresh fruits and vegetables, uncooked spices) that may unduly cause exposure to spores of Aspergillus species or other ubiquitous fungi.
For patients undergoing bone marrow transplantation, solid organ transplantation, or antileukemic chemotherapy, the use of high efficiency particulate air (HEPA) filtration systems in the treatment units may minimize patient risk of exposure to Aspergillus spores.
Administer prophylactic antifungal therapy (ie, treatment with intranasal or intravenous amphotericin B or its other formulations) in patients at high risk for opportunistic fungal infection, including patients with a history of fungal infection. [51]
In a study, prophylactic posaconazole was shown to be superior to fluconazole in reducing invasive aspergillosis incidence (1% vs 5.9%, respectively) in allogeneic hematopoietic stem cell transplant recipients with clinically significant graft-versus-host disease. [52]
In another trial, conducted using neutropenic patients undergoing chemotherapy for acute leukemia or myelodysplasia, prophylactic posaconazole again reduced the incidence of invasive aspergillosis to 1%. The incidence in patients in the study who received either fluconazole or itraconazole was 7%. [53]
Questions & Answers
Overview
Which groups are at increased risk for fungal pneumonia?
How is fungal pneumonia diagnosed?
What are possible complications of fungal pneumonia?
What are the treatment options for fungal pneumonia?
Which occupations increase the risk for fungal pneumonia?
Which medical conditions are risk factors for opportunistic fungal pneumonia?
Where are the fungal pathogens that cause pneumonia most prevalent in the US?
What is the global incidence of fungal pneumonia?
What is the associated morbidity and mortality in fungal pneumonia?
How does the prevalence of fungal pneumonia vary by race?
How does the prevalence of fungal pneumonia vary by sex?
Which body sites are affected by disseminated fungal infections?
What are the signs and symptoms of fungal pneumonia?
What are early signs suggestive of fungal pneumonia?
What are allergic reactions suggestive of fungal pneumonia?
Which signs and symptoms are specific for fungal pneumonia?
What are physical findings suggestive of fungal pneumonia?
What are extrapulmonary findings suggestive of fungal pneumonia?
Which conditions should be included in the differential diagnosis of fungal pneumonia?
Why does the mortality rate for fungal pneumonia remained elevated?
What is the role of lab testing in the workup of fungal pneumonia?
Which WBC count is characteristic of fungal pneumonia?
What does a finding of eosinophilia suggest in the workup of fungal pneumonia?
What does a finding of neutropenia and leukopenia suggest in the workup of fungal pneumonia?
What is the role of sputum cultures in the workup of fungal pneumonia?
What is the role of blood culture in the workup of fungal pneumonia?
What is the role of urine culture in the workup of fungal pneumonia?
What is the role of antigen testing in the workup of fungal pneumonia?
What is the role of serology testing in the workup of fungal pneumonia?
What is the role of radiography in the workup of fungal pneumonia?
What is the role of CT scanning in the workup of fungal pneumonia?
When are CT scans indicated in the workup of fungal pneumonia?
What is the role of MRI in the workup of fungal pneumonia?
What is the role of bronchoscopy in the workup of fungal pneumonia?
What is the role of CT-guided FNA for the workup of fungal pneumonia?
What is the role of open lung biopsy in the workup of fungal pneumonia?
What is the role of lumbar puncture in the workup of fungal pneumonia?
What is the role of bone marrow aspiration in the workup of fungal pneumonia?
Which biopsy findings are characteristic of fungal pneumonia?
Which histologic findings are characteristic of fungal pneumonia?
What are the treatment options for fungal pneumonia?
Which antifungal agents are used in treatment of fungal pneumonia?
What are possible adverse effects of long-term voriconazole treatment for fungal pneumonia?
What is the role of amphotericin B in the treatment of fungal pneumonia?
Which antifungal agents may be alternatives to amphotericin B for treatment of fungal pneumonia?
What is the role of combination therapy in the treatment of fungal pneumonia?
When is surgery indicated for fungal pneumonia?
What are in-patient treatment options for fungal pneumonia?
What monitoring is needed following treatment for fungal pneumonia?
Which specialist consultations are needed for the diagnosis and treatment of fungal pneumonia?
How is fungal pneumonia prevented?
-
Chest radiograph showing multiple pulmonary nodules. The patient was treated with corticosteroids for acute graft versus host disease following bone marrow transplantation for chronic myeloid leukemia. The patient smoked marijuana for 2 weeks prior to this chest radiograph being taken. Bronchoalveolar lavage revealed Aspergillus niger and other species on fungal cultures.
-
CT scan of a patient with invasive aspergillosis showing multiple lung lesions. The cavitary lesion on the left lung shows a ground-glass halo sign.
-
CT scan of aspergillosis of the lungs showing multiple pleural-based and lung parenchymal lesions.
Tables
Fungal Pathogen |
Indication for Antifungal Therapy |
Surgical Care and Other Treatments |
Antifungal Drugs Used |
Acute pulmonary histoplasmosis with hypoxia; prolonged moderate symptoms for more than 1 month; disseminated disease; immunosuppressed host Mortality rate for untreated disseminated disease at 80%; reduced to 25% with treatment |
Significant hemoptysis; recurrent pneumonia; repair of bronchopleural fistula Corticosteroids in severe hypoxia or ARDS Anti-inflammatory agents to treat rheumatologic syndromes |
Amphotericin B induces rapid response in patients who are severely ill or immunocompromised Azoles/triazoles in patients with milder illness |
|
Disseminated disease; chronic pulmonary disease; acute pulmonary infection with hypoxia or protracted morbidity (>1-2 mo); immunosuppressed host (worst outcome, 70% mortality) |
Surgical debridement or resection of infective tissue often necessary adjunct to antifungal treatment Anti-inflammatory agents for rheumatologic syndromes |
Amphotericin B effective in more than 90% of cases; first choice in severe cases or immunocompromised Fluconazole/itraconazole first choice in mild to moderate infection (or after improvement) Treatment less effective than in other endemic mycoses |
|
Persistent or recurrent symptoms of acute or chronic pulmonary disease or with pleural involvement; disseminated disease |
Steroids for ARDS |
Amphotericin B response rates of 77-90% of cases; for severe infection or immunocompromised Itraconazole successful in 90% of cases; for mild to moderate infection Ketoconazole response of 80%; poor outcome in patients who are immunosuppressed Fluconazole less effective, 65% response rate Chronic maintenance treatment essential for all patients with AIDS or meningitis |
|
Patients who are immunosuppressed and symptomatic; patients who are immunocompetent with disease progression; any patients with meningitis or disseminated disease |
N/A |
Amphotericin B in patients who are severely ill Fluconazole in milder cases or after clinical response to amphotericin B Lifelong maintenance therapy in AIDS patients may not be necessary as long as the patient's CD4 count is maintained above 100 cells/µL with HAART [37] Flucytosine may be of benefit when combined with amphotericin B in patients with severe or disseminated disease. [5] |
|
All patients with invasive disease; in patients who are immunosuppressed, early diagnosis and empiric treatment for persistent fever not responding to broad-spectrum antibiotics; high mortality once infiltrates and symptoms appear; prognosis ultimately linked to severity and outcome of underlying disease Mortality rate of 50-60% in patients with AIDS |
Rapid tapering of immunosuppressive agents and corticosteroids and reversal of neutropenia (if possible) |
Voriconazole is the new standard of care for invasive aspergillosis based on superiority over amphotericin B in primary therapy Lipid formulations of amphotericin B have at least equal efficacy but less toxicity compared with amphotericin B desoxycholate Oral voriconazole can be used to complete treatment with initial response to IV voriconazole or amphotericin B Posaconazole is second line agent Echinocandins second line agent when voriconazole is not tolerated or in combination with voriconazole in an attempt to enhance antifungal activity Isavuconazole has been shown to be not inferior to voriconazole for aspergillosis [38] |
|
Mortality rates as high as 70% in patients with invasive pulmonary mucormycosis |
Aggressive surgical debridement of necrotic tissue important in mucormycosis, especially if confined to lungs |
Lipid amphotericin B is the mainstay of therapy; posaconazol is poorly absorbed, considered second line Mucor species generally resistant to azoles (voriconazole has no activity against them) Echinocandins (Caspofungin) useful as salvage therapy Isavuconazole has been shown to be comparable to amphotericin B and posaconazole for mucormycosis [38] |
|
All patients with invasive disease or dissemination; important to reverse factors affecting immune status Expert recommendations and clinical practice guidelines do not recommend antifungal treatment facing isolation in respiratory samples regardless the number of positive samples [15] |
Rapid tapering of immunosuppressive agents and corticosteroids; important to remove indwelling infected intravenous lines or urinary catheters in setting of hematogenous spread |
Amphotericin B is mainstay Flucytosine may be of benefit when added to amphotericin B Fluconazole use in pulmonary disease not studied but is effective in hepatosplenic candidiasis and candidemia Echinocandins may be useful alternatives |
|
Management should be based in clinico-radiological manifestations; two presentations of pulmonary sporotrichosis: non-cavitary disease (multifocal) and cavitary disease (primary) [16] |
Surgical interventions when presence of cavitations and initial medical therapies have failed; used as adjunctive therapy |
Itraconazole as first line agent in mild to moderate cases Amphotericin B first line in life threatening conditions |
|
| Scedosporiosis | Emerging opportunistic pathogen in similar scenario as aspergillosis but highly resistant to amphotericin B and echinocandins; mortality rate is 54-78% in transplant recipients In near-drowning victims, close surveillance for clinical and radiographic findings with low threshold for empiric treatment |
Aggressive surgical debridement for disseminated disease in the form of subcutaneous abscesses, brain abscess, and others Granulocyte transfusions or growth factors to enhance neutrophil recovery |
Resistant to amphotericin B and echinocandins Voriconazole as single agent or in combination with other agents such as terbinafine [39] |

What would you like to print?
- Overview
- Risk Factors
- Epidemiology of Fungal Pneumonia
- Effects of Disseminated Fungal Disease
- Patient History
- Physical Examination
- Differentials in Fungal Pneumonia
- Workup Considerations
- CBC Count With Differential
- Sputum Examination and Potassium Hydroxide Stain
- Blood and Urine Cultures
- Nonculture Methods for Detecting Fungal Infections
- Serology
- Chest Radiography
- CT Scanning and MRI
- Procedures
- Histologic Findings
- Histopathology
- Treatment of Fungal Infection
- Inpatient Considerations
- Outpatient Considerations
- Clinical Consultations
- Deterrence and Prevention of Fungal Pneumonia
- Questions & Answers
- Show All
- Media Gallery
- Tables
- References








