Practice Essentials
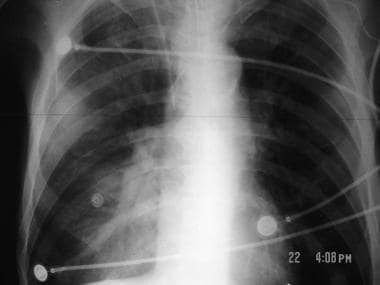
Bacterial pneumonia (see the image below) is caused by a pathogenic infection of the lungs and may present as a primary disease process or as the final, fatal disorder primarily in an individual who is already debilitated. The most consistent presenting symptom of bacterial pneumonia is cough productive of sputum. Antibiotic treatment is the mainstay of drug therapy for bacterial pneumonia.
 Bacterial pneumonia. Radiographic images in a patient with right upper lobe pneumonia. Note the increased anteroposterior chest diameter, which is suggestive of chronic obstructive pulmonary disease (COPD).
Bacterial pneumonia. Radiographic images in a patient with right upper lobe pneumonia. Note the increased anteroposterior chest diameter, which is suggestive of chronic obstructive pulmonary disease (COPD).
Signs and symptoms of bacterial pneumonia
Cough, particularly cough productive of sputum, is the most consistent presenting symptom of bacterial pneumonia and may suggest a particular pathogen, as follows:
-
Streptococcus pneumoniae: Rust-colored sputum
-
Pseudomonas, Haemophilus, and pneumococcal species: May produce green sputum
-
Klebsiella species pneumonia: Red currant-jelly sputum
-
Anaerobic infections: Often produce foul-smelling or bad-tasting sputum
Signs of bacterial pneumonia may include the following:
-
Hyperthermia (fever, typically >38°C) [1] or hypothermia (< 35°C)
-
Tachypnea (>18 respirations/min)
-
Use of accessory respiratory muscles
-
Tachycardia (>100 bpm) or bradycardia (< 60 bpm)
-
Central cyanosis
-
Altered mental status
Physical findings may include the following:
-
Adventitious breath sounds, such as rales/crackles, rhonchi, or wheezes
-
Decreased intensity of breath sounds
-
Egophony
-
Whispering pectoriloquy
-
Dullness to percussion
-
Tracheal deviation
-
Lymphadenopathy
-
Pleural friction rub
Examination findings that may indicate a specific etiology include the following:
-
Bradycardia: May indicate a Legionella etiology
-
Periodontal disease: May suggest an anaerobic and/or polymicrobial infection
-
Cutaneous nodules: May suggest Nocardia infection
-
Decreased gag reflex: Suggests risk for aspiration
See Clinical Presentation for more detail.
Diagnosis of bacterial pneumonia
Severity assessment
Tools to assess the severity of disease and risk of death include the PSI/PORT (ie, pneumonia severity index/Patient Outcomes Research Team score), the CURB-65 (ie, confusion, urea, respiratory rate, blood pressure, and age >65 years) system, and the APACHE (ie, acute physiology and chronic health evaluation), among others.
The following laboratory tests are also useful for assessing illness severity:
-
Serum chemistry panel
-
Arterial blood gas (ABG) determination
-
Venous blood gas determination (central venous oxygen saturation)
-
Complete blood cell (CBC) count with differential
-
Serum free cortisol value
-
Serum lactate level
Sputum evaluation
Sputum Gram stain and culture should be performed before initiating antibiotic therapy. A single predominant microbe should be noted at Gram staining, although mixed flora may be observed with anaerobic infection caused by aspiration.
Imaging studies
-
Chest radiography: The criterion standard for establishing the diagnosis of pneumonia
-
Chest computed tomography scanning
-
Chest ultrasonography
Bronchoscopy
Lung tissue can be visually evaluated and bronchial washing specimens can be obtained with the aid of a fiberoptic bronchoscope. Protected brushings and bronchoalveolar lavage (BAL) can be performed for fluid analysis and cultures.
Thoracentesis
This is an essential procedure in patients with a parapneumonic pleural effusion. Analysis of the fluid allows differentiation between simple and complicated effusions.
Pathogen-specific tests
-
Urine assays
-
Sputum, serum, and/or urinary antigen tests
-
Immune serologic tests
Histologic examination
Histologic inflammatory lung changes vary according to whether the patient has lobar pneumonia, bronchopneumonia, or interstitial pneumonia. [2]
See Workup for more detail.
Management of bacterial pneumonia
The mainstay of drug therapy for bacterial pneumonia is antibiotic treatment. First-line antimicrobials for S pneumoniae, the most prevalent cause of bacterial pneumonia, are, for the penicillin-susceptible form of the bacterium, penicillin G and amoxicillin. For the penicillin-resistant form of S pneumoniae, first-line agents are chosen on the basis of sensitivity.
Supportive measures include the following:
-
Analgesia and antipyretics
-
Chest physiotherapy
-
Intravenous fluids (and, conversely, diuretics), if indicated
-
Pulse oximetry with or without cardiac monitoring, as indicated
-
Oxygen supplementation
-
Positioning of the patient to minimize aspiration risk
-
Respiratory therapy, including treatment with bronchodilators and N-acetylcysteine
-
Suctioning and bronchial hygiene
-
Ventilation with low tidal volumes (6 mL/kg of ideal body weight) in patients requiring mechanical ventilation secondary to bilateral pneumonia or acute respiratory distress syndrome (ARDS) [3]
-
Systemic support: May include proper hydration, nutrition, and mobilization
See Treatment and Medication for more detail.
Background
Pneumonia can be generally defined as an infection of the lung parenchyma, in which consolidation of the affected part and a filling of the alveolar air spaces with exudate, inflammatory cells, and fibrin is characteristic. [4] Infection by bacteria or viruses is the most common cause, although infection by other micro-orgamisms such as rickettsiae, fungi and yeasts, and mycobacteria may occur. [4] (See the images below.)
 A 53-year-old patient with severe Legionella pneumonia. Chest radiograph shows dense consolidation in both lower lobes.
A 53-year-old patient with severe Legionella pneumonia. Chest radiograph shows dense consolidation in both lower lobes.
 A 40-year-old patient with Chlamydia pneumonia. Chest radiograph shows multifocal, patchy consolidation in the right upper, middle, and lower lobes.
A 40-year-old patient with Chlamydia pneumonia. Chest radiograph shows multifocal, patchy consolidation in the right upper, middle, and lower lobes.
 A 38-year-old patient with Mycoplasma pneumonia. Chest radiograph shows a vague, ill-defined opacity in the left lower lobe.
A 38-year-old patient with Mycoplasma pneumonia. Chest radiograph shows a vague, ill-defined opacity in the left lower lobe.
Bacterial pneumonia is caused by a pathogenic infection of the lungs and may present as a primary disease process or as the final coup de grace in the individual who is already debilitated. For example, a historical review of the 1918-19 influenza pandemic suggests that the majority of deaths were not a direct effect of the influenza virus, but they were from bacterial coinfection. [5]
Discussion of bacterial pneumonia involves classification and categorization schemes based on various characteristics of the illness, such as anatomic or radiologic distribution, the setting, or mechanism of acquisition, and the pathogen responsible. A major part of what distinguishes these various categories from each other is the varying risk of exposure to multidrug-resistant (MDR) organisms. [6, 7, 8, 9, 10, 11]
Anatomic or radiologic distribution of pneumonia includes the following (see Chest Radiography for details):
-
Lobar - Known as focal or nonsegmental pneumonia (see the images below)
-
Multifocal/lobular (bronchopneumonia)
-
Interstitial (focal diffuse)
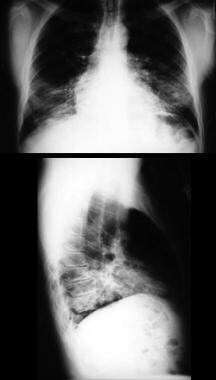
 Bacterial pneumonia. Radiographic images in a patient with right upper lobe pneumonia. Note the increased anteroposterior chest diameter, which is suggestive of chronic obstructive pulmonary disease (COPD).
Bacterial pneumonia. Radiographic images in a patient with right upper lobe pneumonia. Note the increased anteroposterior chest diameter, which is suggestive of chronic obstructive pulmonary disease (COPD).
 Bacterial pneumonia. Radiographic images in a patient with bilateral lower lobe pneumonia. Note the spine sign, or loss of progression of radiolucency of the vertebral bodies
Bacterial pneumonia. Radiographic images in a patient with bilateral lower lobe pneumonia. Note the spine sign, or loss of progression of radiolucency of the vertebral bodies
 Bacterial pneumonia. Radiographic images in a patient with early right middle lobe pneumonia.
Bacterial pneumonia. Radiographic images in a patient with early right middle lobe pneumonia.


The setting of pneumonia includes the community, institutional (healthcare/nursing home setting), and nosocomial (hospital).
Community-acquired pneumonia
Community-acquired pneumonia (CAP) is defined as pneumonia that develops in the outpatient setting or within 48 hours of admission to a hospital.
Go to Community-Acquired Pneumonia for complete information on this topic.
Institutional-acquired pneumonia
Institutional-acquired pneumonia (IAP) includes HCAP and nursing home–associated pneumonia (NHAP).
HCAP is defined as pneumonia that develops in the outpatient setting or within 48 hours of admission to a hospital in patients with increased risk of exposure to MDR bacteria as a cause of infection. Risk factors for exposure to MDR bacteria in HCAP include the following:
-
Hospitalization for two or more days in an acute care facility within 90 days of current illness
-
Exposure to antibiotics, chemotherapy, or wound care within 30 days of current illness
-
Residence in a nursing home or long-term care facility
-
Hemodialysis at a hospital or clinic
-
Home nursing care (infusion therapy, wound care)
-
Contact with a family member or other close person with infection due to MDR bacteria
NHAP is generally included in the category of HCAP because of the high incidence of infection with gram-negative bacilli and Staphylococcus aureus. However, some authors accept NHAP as a separate entity because of distinct epidemiologic associations with infection in nonhospital healthcare settings. [4] Pneumonia in patients in nursing homes and long-term care facilities has been associated with greater mortality than in patients with CAP. These differences may be due to factors such as disparities in functional status, likelihood of exposure to infectious agents, and variations in pathogen virulence, among others.
It is important to note that nursing home patients with pneumonia are less likely to present with classic signs and symptoms of the typical pneumonia presentation, such as fever, chills, chest pain, and productive cough, but instead these individuals often have delirium and altered mental status. [6, 7]
Go to Nursing Home Acquired Pneumonia for complete information on this topic.
The concept of HCAP (including NHAP) has been called into question in the 2016 Infectious Diseases Society of America (IDSA) and American Thoracic Society (ATS) guidelines. [12] Based on a 2014 meta-analysis of 24 studies, it was found that the concept of HCAP is predominantly based on low-quality evidence confounded by publication bias and does not accurately identify multidrug-resistant organisms. After adjusting for age and comorbidities, patients within this category did not have an increased risk of mortality. [13] Based on this meta-analysis, the 2016 IDSA and ATS guidelines have called for the removal of the concept of HCAP, [12] encouraging patients previously grouped under this category to be treated as if they have CAP, with guidance of hospital-specific antibiograms and local resistance patterns.
Nosocomial pneumonia
Nosocomial infections are generally described as those acquired in the hospital setting. The term nosocomial pneumonia has evolved into the more succinct clinical entities of hospital-acquired pneumonia (HAP) and ventilator-associated pneumonia (VAP). However, the term nosocomial pneumonia still has an appropriate place in the descriptive language of pneumonia. Nosocomial infections have been viewed as a "tribute to pay to the more aggressive management of the population, characterized by the use of sophisticated technologies and invasive devices," an important consideration in the pulmonary care of critically ill patients. [14]
Go to Ventilator-Associated Pneumonia and Nosocomial Pneumonia for complete information on these topics.
Hospital-acquired pneumonia
HAP is defined as pneumonia that develops at least 48 hours after admission to a hospital and is characterized by increased risk of exposure to MDR organisms, [6] as well as gram-negative organisms. [15] Risk factors for exposure to such organisms in HAP include the following [6] :
-
Antibiotic therapy within 90 days of the hospital-acquired infection
-
Current length of hospitalization of five days or more
-
High frequency of antibiotic resistance in the local community or within the specific hospital unit
-
Immunosuppressive disease or therapy
-
Presence of HCAP risk factors for exposure to MDR bacteria
Common mechanisms for the acquisition of pneumonia include ventilator use and aspiration.
Ventilator-associated pneumonia
VAP is defined as pneumonia that develops more than 48 hours after endotracheal intubation or within 48 hours of extubation. Risk factors for exposure to MDR bacteria that cause VAP are the same as those for HAP. [6, 8] VAP may occur in as many as 10-20% of patients who are on ventilators for more than 48 hours. [16]
Go to Ventilator-Associated Pneumonia for complete information on this topic.
Aspiration pneumonia
Aspiration pneumonia develops after the inhalation of oropharyngeal secretions and colonized organisms. Although organisms frequently implicated in CAP, such as Haemophilus influenzae and Streptococcus pneumoniae, can colonize the nasopharynx and oropharynx and their aspiration can contribute to the development of CAP, the term aspiration pneumonia refers specifically to the development of an infectious infiltrate in patients who are at increased risk of oropharyngeal aspiration.
Patients may be at increased risk of aspiration and/or the development of aspiration pneumonia for a number of reasons, as follows:
-
Decreased ability to clear oropharyngeal secretions - Poor cough or gag reflex, impaired swallowing mechanism (eg, dysphagia in stroke patients), impaired ciliary transport (eg, from smoking)
-
Increased volume of secretions
-
Increased bacterial burden of secretions
-
Presence of other comorbidities - Anatomic abnormalities, gastroesophageal reflux disease (GERD), achalasia.
Critically ill patients are at notably increased risk of aspiration due to the following:
-
The challenge of appropriate, risk-minimizing positioning
-
Gastroparesis/dysmotility
-
Impaired cough/gag/swallow reflexes (illness- or drug-induced)
-
Impaired immune response
-
Intubation/extubation
Historically, the bacteria implicated in aspiration pneumonia have been the anaerobic oropharyngeal colonizers such as Peptostreptococcus, Bacteroides, Fusobacterium, and Prevotella species. However, now evident is that the vast majority of cases of aspiration pneumonia result from the same pathogens implicated in CAP and HAP, depending on the setting in which the aspiration event occurred. The clinical course of aspiration pneumonia is, thus, similar to that of CAP or HAP. [17] However, recurrence of aspiration pneumonia is common unless the risk factors for underlying aspiration are treated or minimized.
Go to Aspiration Pneumonia for complete information on this topic.
Pathophysiology
The causes for the development of pneumonia are extrinsic or intrinsic, and various bacterial causes are noted. Extrinsic factors include exposure to a causative agent, exposure to pulmonary irritants, or direct pulmonary injury. Intrinsic factors are related to the host. Loss of protective upper airway reflexes allows aspiration of contents from the upper airways into the lung. Various causes for this loss include altered mental status due to intoxication and other metabolic states and neurologic causes, such as stroke and endotracheal intubation.
Bacteria from the upper airways or, less commonly, from hematogenous spread, find their way to the lung parenchyma. Once there, a combination of factors (including virulence of the infecting organism, status of the local defenses, and overall health of the patient) may lead to bacterial pneumonia. The patient may be made more susceptible to infection because of an overall impairment of the immune response (eg, human immunodeficiency virus [HIV] infection, chronic disease, advanced age) and/or dysfunction of defense mechanisms (eg, smoking, chronic obstructive pulmonary disease [COPD], tumors, inhaled toxins, aspiration). Poor dentition or chronic periodontitis is another predisposing factor.
Thus, during pulmonary infection, acute inflammation results in the migration of neutrophils out of capillaries and into the air spaces, forming a marginated pool of neutrophils that is ready to respond when needed. These neutrophils phagocytize microbes and kill them with reactive oxygen species, antimicrobial proteins, and degradative enzymes. They also extrude a chromatin meshwork containing antimicrobial proteins that trap and kill extracellular bacteria, known as neutrophil extracellular traps (NETs). Various membrane receptors and ligands are involved in the complex interaction between microbes, cells of the lung parenchyma, and immune defense cells. [18]
Bacterial virulence
General mechanisms of increased virulence include the following:
-
Genetic flexibility allowing the development of resistance to various classes of antibiotics
-
Flagellae and other bacterial appendages that facilitate spread of infection
-
Capsules resistant to attack by immune defense cells and that facilitate adhesion to host cells
-
Quorum sensing systems allow coordination of gene expression based on complex cell-signaling for adaptation to the local cellular environment
-
Iron scavenging
The following are examples of organism-specific virulence factors:
-
Streptococcus pneumoniae – Pneumolysin, a multifunctional virulence factor, is cytotoxic to respiratory epithelium and endothelium by disrupting pulmonary tissue barriers. This factor directly inhibits immune and inflammatory cells and activates complement, decreasing the clearance of the bacteria from the lung. [19]
-
Pseudomonas aeruginosa - Pili play important role in the attachment to host cells. A type III secretion system allows injection of toxins into host cells. [20]
Host resistance
Deficits in various host defenses and an inability to mount an appropriate acute inflammatory response can predispose patients to infection, as follows [18] :
-
Deficits in neutrophil quantity, as in neutropenia
-
Deficits in neutrophil quality, as in chronic granulomatous disease
-
Deficiencies of complement
-
Deficiencies of immunoglobulins
Viral infection
With the recent H1N1 influenza virus pandemic, it is important to address the role that viral infection can have in bacterial pneumonia.
The association between infection with influenza virus and subsequent bacterial pneumonia became particularly apparent following the 1918 influenza pandemic, during which approximately 40-50 million people died. [21] Historical investigations and current researchers argue that the vast majority of pulmonary-related deaths from past pandemic influenza viruses, most notably the pandemic of 1918, ultimately resulted from bacteriologic secondary or coinfection and poorly understood interactions between the infecting viral and bacterial organisms. [22] Although influenza virus is the most commonly thought of agent in this co-infective context, other respiratory viruses, such as respiratory syncytial virus (RSV), parainfluenza viruses, adenovirus, and rhinoviruses, may also predispose to secondary bacterial infection. [21]
The classic explanation behind the viral-bacterial interplay focuses on the disruption of the respiratory epithelium by the virus, providing an opportinistic environment for bacterial infection. However, evidence depicts much more complex and possibly synergistic interactions between viruses and bacteria, including alteration of pulmonary physiology, downregulation of the host immune defense, changes in expression of receptors to which bacteria adhere, and enhancement of the inflammatory process. [21]
Etiology of Bacterial Pneumonia
Although pneumonia may be caused by myriad pathogens, a limited number of agents are responsible for most cases, [3, 23, 24, 25] Most authors categorize bacterial pneumonias by their infectious agents, which include pneumococcal agents; Haemophilus influenzae; Klebsiella, Staphylococcus, and Legionella species; gram-negative organisms; and aspirated micro-organisms. Microaspiration of organisms that colonize the upper respiratory tract and mucosal surfaces is probably the most common mode of infection. Some agents, notably Staphylococcus species, may be spread hematogenously.
Risk factors
Coinfection with H1N1 influenza increases the risk of secondary bacterial pneumonia, with S pneumoniae the most likely coinfection. [26] However, pregnant patients with H1N1 influenza in the 2009 pandemic were at increased risk of developing secondary Klebsiella pneumonia with poor clinical outcome. [27]
Other risk factors include local lung pathologies (eg, tumors, chronic obstructive pulmonary disease [COPD], bronchiectasis), chronic gingivitis and periodontitis, and smoking which impairs resistance to infection. Furthermore, any individual with an altered sensorium (eg, seizures, alcohol or drug intoxication) or central nervous system (CNS) impairment (eg, stroke) may have a reduced gag reflex, which allows aspiration of stomach or oropharyngeal contents and contributes to the development of aspiration pneumonias.
Typical organisms
Although several of the organisms discussed in this section may be implicated in pneumonia, only a few of them are responsible for the vast majority of cases.
Gram-positive bacteria that can cause pneumonia include the following:
-
Streptococcus pneumoniae: This organism is a facultative anaerobe identified by its chainlike staining pattern. Pneumococcosis is by far the most common cause of typical bacterial pneumonia.
-
Staphylococcus aureus: S aureus is a facultative anaerobe identified by its clusterlike staining pattern. S aureus pneumonia is observed in intravenous drug abusers (IVDAs) and individuals with debilitating disorders. In patients who abuse intravenous drugs, the infection probably is spread hematogenously to the lungs from contaminated injection sites. Methicillin-resistant S aureus (MRSA) has had a large impact on empiric antibiotic choices at many institutions.
-
Enterococcus (E faecalis, E faecium): These organisms are group D streptococci that are well-known normal gut florae that can be identified by their pair-and-chain staining pattern. The emergence of vancomycin-resistant Enterococcus (VRE) is indicative of the importance of appropriate antibiotic use.
-
Actinomyces israelii: This is a beaded, filamentous anaerobic organism that grows as normal flora in the gastrointestinal (GI) tract and can colonize the oral cavity in patients with periodontal disease. A israelii is known to form abscesses and sulfur granules.
-
Nocardia asteroides: N asteroides is a weakly gram-positive, partially acid-fast bacillus (AFB) that forms beaded, branching, thin filaments. It is known to cause lung abscesses and cavitations. Erosion into the pleura can also occur, resulting in hematologic spread of the organism.
Gram-negative pneumonias occur most often in individuals who are debilitated, immunocompromised, or recently hospitalized. Individuals living in long-term care facilities where other residents are intubated are also at risk for these infections. Gram-negative bacteria include the following:
-
Pseudomonas aeruginosa: P aeruginosa is an aerobic, motile bacillus often characterized by its distinct (grapelike) odor.
-
Klebsiella pneumoniae: K pneumoniae is a facultatively anaerobic, encapsulated bacillus that can lead to an aggressive, necrotizing, lobar pneumonia. Patients with chronic alcoholism, diabetes, or COPD are at increased risk for infection with this organism.
-
Haemophilus influenzae: H influenzae is an aerobic bacillus that comes in both encapsulated and nonencapsulated forms. Several major subtypes have been identified, which have varying levels of pathogenicity. Encapsulated type B (HiB) is known to be particularly virulent, although routine vaccination against this subtype has decreased the prevalence of severe disease caused by H influenzae. Infection with this bacteria is more common in patients with COPD.
-
Escherichia coli: E coli is a facultatively anaerobic, motile bacillus. It is well known to colonize the lower GI tract and produce the essential vitamin K.
-
Moraxella catarrhalis: M catarrhalis is an aerobic diplococcus known as a common colonizer of the respiratory tract.
-
Acinetobacter baumannii: A baumannii is a pathogen that has been well described in the context of ventilator-associated pneumonia (VAP).
-
Francisella tularensis: F tularensis is the causative agent of tularemia or rabbit fever. F tularensis is a facultative intracellular bacterium that multiplies within macrophages and that is typically transmitted to humans via a tick bite. Its reservoir animals include rodents, rabbits, and hares. F tularensis can also be transmitted in an airborne manner or contracted from handling dead, infected animals. It is commonly spoken of in terms of its potential use as a biologic weapon. [28]
-
Bacillus anthracis: B anthracis is the agent responsible for inhalational anthrax.
-
Yersinia pestis: Y pestis infection is better known as the black plague. It is the most commonly accepted cause of the pandemic known as the bubonic plague. This organism can also cause the pneumonic plague. The pneumonic plague causes a lung infection by the direct inhalation of aerosolised plague bacteria or, secondary, when the organism spreads to the lungs from the bloodstream. Pneumonic plague is, therefore, not exclusively vector-borne like bubonic plague. Instead, it can be spread from person to person. Other members of the Yersinia family are responsible for a wide variety of infectious presentations.
Atypical organisms
Atypical organisms are generally associated with a milder form of pneumonia, the so-called "walking pneumonia." A feature that makes these organisms atypical is the inability to detect them on Gram stain or to cultivate them in standard bacteriologic media. [23, 3] Atypical organisms include the following:
-
Mycoplasma species: The mycoplasmas are the smallest known free-living organisms in existence. These organisms lack cell walls (and therefore are not apparent after Gram stain) but have protective 3-layered cell membranes.
-
Chlamydophila species (C psittaci, C pneumoniae): Psittacosis, also known as parrot disease or parrot fever, is caused by C psittaci and is associated with the handling of various types of birds.
-
Legionella species: Legionella species are gram-negative bacteria found in freshwater and are known to grow in complex water distribution systems. Institutional water contamination is frequently noted in endemic outbreaks. Legionellapneumophila is the causative agent of the majority of Legionnaires' disease. Other Legionella species are known to infect the lower respiratory system.
-
Coxiella burnetii:C burnetii is the causative agent of Q fever. It is spread from animals to humans; person-to-person transmission is unusual. Animal reservoirs typically include cats, sheep, and cattle.
-
Bordetella pertussis:B pertussis is the agent responsible for pertussis or whooping cough.
Anaerobic organisms
Pneumonia due to anaerobes typically results from aspiration of oropharyngeal contents, as previously mentioned. These infections tend to be polymicrobial and may consist of the following anaerobic species, some of which have already been discussed above: Klebsiella, Peptostreptococcus, Bacteroides, Fusobacterium, and Prevotella.
Epidemiology
In the United States, acute lower respiratory tract infections cause more disease and death than any other infection. [18] In fact, these infections also cause a greater burden of disease worldwide than human immunodeficiency virus (HIV) infection, malaria, cancer, or heart attacks. [18] The prevalence of various pathogens and epidemiology of disease vary widely between countries and regions, making precise discussion of international disease burden difficult.
More than three million cases occur annually in the United States. Pneumonia is more prevalent during the winter months and in colder climates. This condition is most likely from viral upper and lower respiratory infections, which increase in winter and result in impaired host defenses to bacterial superinfection.
Community-acquired pneumonia
The most common etiologies of community-acquired pneumonia (CAP) in the outpatient setting are as follows (in descending order of frequency): [3] S pneumoniae, M pneumoniae, H influenzae, C pneumoniae, and respiratory viruses.
The most common etiologies of CAP in the non–intensive care unit (ICU) inpatient setting, in descending order of frequency, are as follows: [3] S pneumoniae, M pneumoniae, C pneumoniae, H influenzae, Legionella species, aspiration, and respiratory viruses. Legionella pneumophila infections tend to occur sporadically and in local epidemic clusters. These infections usually arise in the summer and fall and may be found in the water condensed from air conditioning systems.
The most common etiologies of CAP in the ICU inpatient setting, in descending order of frequency, are as follows [3] : S pneumoniae, S aureus, Legionella species, and Gram-negative bacilli.
Ventilator-associated pneumonia (VAP) notably develops in approximately 9-27% of all intubated patients and carries a mortality rate of 30-60%. [8, 29]
Race, sex, and age
Black men (26.6 deaths per 100,000 population) are more likely to die from pneumonia compared with white men (23 deaths per 100,000 population), whereas black (17.4 deaths per 100,000 population) and white women (18.2 deaths per 100,000 population) are almost equally likely to die from pneumonia. [30, 31]
The incidence of pneumonia is greater in males than in females but the total number of deaths due to pneumonia has been higher among females since the mid 1980s. However, females have age-adjusted death rates close to 30% lower than those in men, because the female population in the United States is larger than the male population. The age-adjusted death rates for females have been reported as 17.9 deaths per 100,000 population and 23.9 deaths per 100,000 population for males. [30, 31]
Advanced age increases the incidence of and the mortality from pneumonia. Comorbidity and a diminished immune response and defense against aspiration increase the risk of bacterial pneumonia. For individuals aged 65 years and older, pneumonia and influenza were the sixth leading cause of death in 2005. [30, 31] Close to 90% of deaths due to pneumonia and influenza occurred in this age group. In a 20-year US study, the average overall mortality rate in pneumococcal pneumonia with bacteremia was 20.3%. Patients older than 80 years of age had the highest mortality rate, which was 37.7%. [32]
Prognosis
Generally, the prognosis is good in otherwise healthy patients with uncomplicated pneumonia. Advanced age, aggressive organisms (eg, Klebsiella, Legionella, resistant S pneumoniae), comorbidity, respiratory failure, neutropenia, and features of sepsis, alone or in combination, increase morbidity and mortality. Left untreated, pneumonia may have an overall mortality rate of more than 30%.
Even with appropriate treatment, the risk of mortality may be high if the host is ill or infirm. The Pneumonia Severity Index (PSI) may be used as a guide to determine a patient's mortality risk, but it tends to overestimate the actual risk in many cases (see Pneumonia severity index under Risk Stratification in Clinical Presentation). Particularly virulent organisms, such as Klebsiella and Legionella species, may confer a higher mortality rate.
In a study looking at microbial etiologies of CAP, S pneumoniae was present in the highest total number of deaths. However, gram-negative enteric bacilli, Pseudomonas, Staphylococcus aureus, and mixed etiologies had the highest mortality rates in those effected. [33]
Morbidity may include destruction of lung tissue from infection with subsequent scarring. Affected areas may be incapable of gas exchange, reducing respiratory reserve. In a patient with pre-existing respiratory disease, the onset of bacterial pneumonia may result in a downward spiral of infections, further impairment of respiratory status, and repeated infections owing to reduced local and systemic immune responses. Bronchiectasis may be a sequela of bacterial pneumonia. Infections with Staphylococcus and Klebsiella organisms may result in subsequent bronchiectasis, especially if treatment is delayed.
Destroyed alveoli and small-to-medium airways may be replaced by dilated blind saccules filled with purulent material. Ongoing, chronic inflammation usually occurs in the surrounding area and may destroy local adjacent lung tissue over time. Empyema and lung abscess may occur as direct complications of bacterial pneumonia. Pneumonia has been associated with increased incidence of placental abruption in pregnant patients.
Patient Education
Patients should be encouraged to stop smoking, to avoid drinking alcohol to intoxication, and to keep their teeth in good repair. In addition, instruct patients at risk to receive appropriate influenza and pneumococcal immunizations.
Patients, particularly elderly and debilitated patients, should be instructed to seek prompt care should symptoms of dyspnea or fever and rigors develop.
For patient education information, see the Lungs Center, as well as Bacterial Pneumonia and Viral Pneumonia.
-
Bacterial pneumonia. Radiographic images in a patient with right upper lobe pneumonia. Note the increased anteroposterior chest diameter, which is suggestive of chronic obstructive pulmonary disease (COPD).
-
Bacterial pneumonia. Radiographic images in a patient with bilateral lower lobe pneumonia. Note the spine sign, or loss of progression of radiolucency of the vertebral bodies
-
Bacterial pneumonia. Radiographic images in a patient with early right middle lobe pneumonia.
-
A 53-year-old patient with severe Legionella pneumonia. Chest radiograph shows dense consolidation in both lower lobes.
-
A 40-year-old patient with Chlamydia pneumonia. Chest radiograph shows multifocal, patchy consolidation in the right upper, middle, and lower lobes.
-
A 38-year-old patient with Mycoplasma pneumonia. Chest radiograph shows a vague, ill-defined opacity in the left lower lobe.
-
Chest computed tomography scan shows ill-defined, airspace infiltrate in the left lower lobe.
-
Chest computed tomography scan in a 45-year-old patient with Chlamydia pneumonia shows a right upper-lobe infiltrate.
-
Image in a 49-year-old woman with pneumococcal pneumonia. The chest radiograph reveals a left lower lobe opacity with pleural effusion.
-
Image in a 48-year-old patient with Haemophilus influenzae pneumonia. The chest radiograph shows bilateral opacities with a predominantly peripheral distribution.
-
Image in a 49-year-old patient with pneumococcal pneumonia. This chest CT shows a left upper lobe opacity extending to the periphery.
-
Image in a 50-year-old patient with Haemophilus influenzae pneumonia. The chest CT shows a very dense round area of consolidation adjacent to the pleura in the left lower lobe.
-
(Left) Gram stain demonstrating gram-positive cocci in pairs and chains and (right) culture positive for Streptococcus pneumoniae.
-
Gram stain showing Streptococcus pneumoniae.
-
Gram stain showing Haemophilus influenzae.
-
Gram stain showing Moraxella catarrhalis.
-
Sputum direct fluorescent antibody stain showing Legionella infection.
-
Chest radiograph in a patient with HIV infection, bilateral perihilar infiltrates, and Pneumocystis jiroveci pericarditis.
-
Chest radiograph in a patient with HIV infection and focal infiltrates due to tuberculosis.
Tables
Organism |
First-Line Antimicrobials |
Alternative Antimicrobials |
|
Streptococcus pneumoniae |
|||
|
Penicillin susceptible (MIC < 2 mcg/mL) |
Penicillin G, amoxicillin |
Macrolide, cephalosporin (oral or parenteral), clindamycin, doxycycline, respiratory fluoroquinolone |
|
Penicillin resistant (MIC ≥2 mcg/mL) |
Agents chosen on the basis of sensitivity |
Vancomycin, linezolid, high-dose amoxicillin (3 g/d with MIC ≤4 mcg/mL |
Staphylococcus aureus |
|||
|
Methicillin susceptible |
Antistaphylococcal penicillin |
Cefazolin, clindamycin |
|
Methicillin resistant |
Vancomycin, linezolid |
Trimethoprim- sulfamethoxazole |
Haemophilus influenzae |
|||
|
Non–beta-lactamase producing |
Amoxicillin |
Fluoroquinolone, doxycycline, azithromycin, clarithromycin |
|
Beta-lactamase producing |
Second- or third-generation cephalosporin, amoxicillin/clavulanate |
Fluoroquinolone, doxycycline, azithromycin, clarithromycin |
Mycoplasma pneumoniae |
Macrolide, tetracycline |
Fluoroquinolone |
|
Chlamydophila pneumoniae |
Macrolide, tetracycline |
Fluoroquinolone |
|
Legionella species |
Fluoroquinolone, azithromycin |
Doxycycline |
|
Chlamydophila psittaci |
Tetracycline |
Macrolide |
|
Coxiella burnetii |
Tetracycline |
Macrolide |
|
Francisella tularensis |
Doxycycline |
Gentamicin, streptomycin |
|
Yersinia pestis |
Streptomycin, gentamicin |
Doxycycline, fluoroquinolone |
|
Bacillus anthracis (inhalational) |
Ciprofloxacin, levofloxacin, doxycycline |
Other fluoroquinolones, beta-lactam (if susceptible), rifampin, clindamycin, chloramphenicol |
|
Enterobacteriaceae |
Third-generation cephalosporin, carbapenem |
Beta-lactam/beta-lactamase inhibitor, fluoroquinolone |
|
Pseudomonas aeruginosa |
Antipseudomonal beta-lactam plus ciprofloxacin, levofloxacin, or aminoglycoside |
Aminoglycoside plus ciprofloxacin or levofloxacin |
|
Bordetella pertussis |
Macrolide |
Trimethoprim- sulfamethoxazole |
|
Anaerobe (aspiration) |
Beta-lactam/beta-lactamase inhibitor, clindamycin |
Carbapenem |
|
MIC = Minimal inhibitory concentration. |
|||

What would you like to print?
- Overview
- Presentation
- DDx
- Workup
- Treatment
- Medication
- Medication Summary
- Fluoroquinolones
- Cephalosporins
- Macrolides
- Monobactams
- Antibiotics, Lincosamide
- Tetracyclines
- Carbapenems
- Oxazolidinones
- Aminoglycosides
- Penicillins, Amino
- Penicillins, Extended-Spectrum
- Penicillins, Natural
- Sulfonamides
- Glycopeptides
- Pleuromutilin
- Glucocorticoids
- Vaccines
- Show All
- Questions & Answers
- Media Gallery
- Tables
- References








