Practice Essentials
Pneumococcal infections are caused by Streptococcus pneumoniae, a lancet-shaped, gram-positive, catalase-negative facultative anaerobe commonly referred to as pneumococcus. S pneumoniae is the most common cause of community-acquired pneumonia (CAP), bacterial meningitis, bacteremia, and otitis media, as well as an important cause of sinusitis, septic arthritis, osteomyelitis, peritonitis, and endocarditis. Complications of each of these diagnoses are common. See the image below. Clinical signs and symptoms and physical examination findings alone cannot distinguish S pneumoniae disease from infections caused by other pathogens.
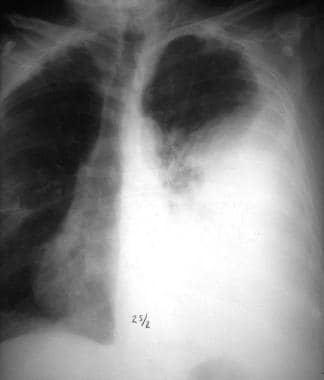 Empyema caused by Streptococcus pneumoniae. Anteroposterior film. Courtesy of R. Duperval, MD.
Empyema caused by Streptococcus pneumoniae. Anteroposterior film. Courtesy of R. Duperval, MD.
Epidemiology
S pneumoniae can cause a wide variety of clinical symptoms owing to its ability to cause disease by either direct extension from the nasopharynx into surrounding anatomic structures or vascular invasion with hematogenous spread. Features that should prompt the clinician to consider pneumococcal infection include the following:
-
High-risk age groups (children younger than 5 years, particularly aged 2 years or younger; adults older than 55-65 years)
-
Conditions that cause immune deficits (eg, HIV infection, malignancy, or diabetes mellitus)
-
Conditions associated with decreased pulmonary clearance functions (eg, asthma, chronic bronchitis, or chronic obstructive pulmonary disease [COPD])
-
Presentation from late fall to early spring
Conditions that may develop by direct extension of S pneumoniae from the nasopharynx include the following:
-
Conjunctivitis
-
Otitis media
-
Sinusitis
-
Acute exacerbations of chronic bronchitis (AECB)
-
Pneumonia (which may be complicated by purulent pericarditis)
Conditions that may result from vascular invasion and hematogenous spread of S pneumoniae include the following:
-
Meningitis
-
Bacteremia (most common manifestation of invasive pneumococcal disease)
-
Joint and bone infections (osteomyelitis and septic arthritis)
-
Soft tissue infections (eg, myositis, periorbital cellulitis, abscess)
-
Peritonitis
-
Cardiac infections (eg, endocarditis)
See Clinical Presentation for more detail.
Diagnosis
If a pneumococcal infection is suspected or considered, Gram stain and culture of appropriate specimens should be obtained, when possible. Potential specimens may include 1 or more of the following:
-
Blood
-
Cerebrospinal fluid
-
Sputum
-
Pleural fluid or lung aspirate
-
Joint fluid
-
Bone
-
Other abscess or tissue specimens
All S pneumoniae isolates, regardless of the isolation site, should be tested for susceptibility to penicillin and cefotaxime or ceftriaxone. Susceptibilities based on the type of specimen (CSF versus other) were defined by the Clinical and Laboratory Institute (CLSI) in 2008. [1, 2]
Nonspecific laboratory tests that may support the diagnosis include the following:
-
Complete blood count and differential
-
Erythrocyte sedimentation rate (ESR)
-
C-reactive protein (CRP)
Imaging studies that may be helpful include the following:
-
Chest radiography
-
Ultrasonography of the chest
-
Computed tomography (CT) of the chest, sinuses, face, or affected bones or joints
-
Magnetic resonance imaging (MRI) of the brain (in meningitis) or affected bones and joints
Other modalities that may help define the extent of infection include the following:
-
Echocardiography
-
Middle-ear fluid aspiration
-
Pleural fluid aspiration
-
Chest tube thoracostomy or catheter placement
-
Video-assisted thoracoscopy (VATS) or pleural decortication
-
Joint fluid aspiration
-
Biopsy of bone, soft tissue, or muscle
See Workup for more detail.
Management
Antibiotics are the mainstay of therapy. Treatments for specific infections may include the following:
-
Otitis media: In most cases, amoxicillin 80-90 mg/kg/day; if there is no improvement within 48-72 hours, amoxicillin-clavulanate or a second- or third-generation oral cephalosporin (or parenteral ceftriaxone for highly resistant pneumococci)
-
Sinusitis: Initial recommendations as for otitis media; in adult penicillin-allergic patients and patients who do not respond to initial therapy, switching to fluoroquinolones (not approved for children in this clinical situation) may be considered
-
Pneumonia: For penicillin-sensitive S pneumoniae (minimum inhibitory concentration [MIC] < 2 μg/mL), penicillin G or amoxicillin is considered first-line therapy; for penicillin-resistant S pneumoniae infection (MIC ≥2 μg/mL), the choice of antimicrobial agent should be directed by susceptibility testing [3]
-
Meningitis: In children, a beta-lactam (penicillin, ceftriaxone, or cefotaxime) with or without vancomycin pending susceptibility testing; children with hypersensitivity to beta-lactams should receive vancomycin plus rifampin; meropenem and chloramphenicol also have been used; for adults with penicillin-sensitive S pneumoniae infection (MIC ≤ 0.06 μg/mL), intravenous penicillin G or ampicillin is first-line therapy; for penicillin-resistant pneumococcus (MIC ≥0.12 μg/mL), treatment with a third-generation cephalosporin (if ceftriaxone or cefotaxime MIC < 1 μg/mL) or a third-generation cephalosporin plus vancomycin (if cefotaxime or ceftriaxone MIC ≥1 μg/mL) is recommended
Additional treatment measures that may be helpful for particular conditions are as follows:
-
Complicated pneumonia: Chest tube placement for drainage of pleural fluid; in more severe cases, VATS or decortication
-
Suspected septic arthritis or osteomyelitis: Collection of appropriate specimens for Gram stain, cell count, histology, or culture
-
Recurrent or chronic otitis media, periorbital or orbital cellulitis, or facial cellulitis: Surgical intervention
Measures for preventing pneumococcal infection include the following:
-
Behavior modification and risk factor reduction
-
Medical therapy
-
Antimicrobial prophylaxis (in selected patients) with recurrent otitis media.
-
Immunization
See Treatment and Medication for more detail.
Background
S pneumoniae is a gram-positive, catalase-negative coccus that has remained an extremely important human bacterial pathogen since its initial recognition in the late 1800s. The term pneumococcus gained widespread use by the late 1880s, when it was recognized as the most common cause of bacterial lobar pneumonia.
Worldwide, S pneumoniae remains the most common bacterial cause of community-acquired pneumonia (CAP). A recent study showed that 38% of CAP cases were pinpointed to a specific pathogen; out of these, one or more viruses were retrieved in 23% of cases and bacteria in 11%, with a combination seen in 3%. Fungal and mycobacterial organisms accounted for 1%. Human rhinoviruses were isolated in 9% of cases and influenza virus in 6%. S pneumoniae remained the most common cause of bacterial CAP, at 5% of patients. [4]
S pneumoniae is a common cause of bacterial meningitis, bacteremia, and otitis media. S pneumoniae infection is also an important cause of sinusitis, septic arthritis, osteomyelitis, peritonitis, and endocarditis. Worldwide in 2000, 14.5 million estimated episodes of invasive pneumococcal disease were reported in children younger than 5 years, which correlates to more than 800,000 estimated deaths (11% of all deaths in this age group). [5]
The first pneumococcal vaccine was released in 1977, made from polysaccharides from seven serotypes of S pneumoniae. In 1983 a new vaccine came out with 23 serotypes (PPSV23) and largely replaced the first. The first conjugate vaccine was released in 2000 (PCV7). In the early 2000s, studies showed that routine vaccination led to decreased rates of invasive pneumococcal infections (>90%) caused by pneumococcal serotypes covered by the vaccine, as well as overall decreased rates of invasive disease (45% overall; 75% in children < 5 years). In children younger than 5, surveillance data showed a 100% reduction in invasive disease caused by the 7 serotypes covered in PCV7. In addition, herd immunity has led to decreased rates of disease in older children and adults. [6, 7, 8]
An analysis of 653 invasive pneumococcal infections in the Spanish population before and after the implementation of PCV7 immunization showed an increased incidence of invasive disease in the postvaccine period, which primarily was due to nonvaccine serotypes and was associated with higher rates of complications, such as septic shock. Similar studies in the United States and other European countries have shown similar results, introducing the concept of replacement disease and its effects.
Serotype 19A has received the most attention, not only because of increased disease rates associated with this serotype, but also owing to its association with increased drug resistance. Increased rates of invasive disease with such serotypes caused the overall rates of invasive disease to remain somewhat steady starting in 2002, although these rates remain greatly reduced from rates prior to introduction of the conjugate vaccine.
For these reasons, work on the development of a vaccine containing additional serotypes continued. A 13-valent PCV (PCV13) was approved by the US Food and Drug Administration (FDA) on February 24, 2010 with the hope that its induced T-cell–dependent immune response would have increased efficacy in children and elderly persons. This potential benefit has yet to be demonstrated in elderly individuals. [6, 9, 10, 11, 12, 13, 14, 15, 8, 16, 17, 18, 5, 19, 20]
The 23-valent polysaccharide vaccine is more effective in decreasing pneumococcal bacteremia than pneumonia. As a result, mortality rates have decreased. Ongoing surveillance will help determine the effects of widespread routine immunization with PCV13 and its expanded serotype coverage on pneumococcal disease in children and adults.
In January 2013, the FDA approved PCV13 for the prevention of invasive pneumococcal disease in children and adolescents between 6 and 17 years of age. [21] In February 2013, the CDC's Advisory Committee on Immunization Practices (ACIP) voted for the use of the vaccine in children with immunodeficiencies. The panel recommends routine use of a single dose of PCV13 for children aged 6-18 years who have an immunocompromising condition (eg, sickle cell disease or HIV infection) and have not previously received the vaccine. [22]
Despite an overall decreased incidence of otitis media caused by serotypes covered by vaccination since the introduction of the conjugate pneumococcal vaccine, an increase in rates of disease caused by serotypes not covered by the vaccine has occurred, as well as an increase in rates of diseases caused by vaccine-covered serotypes in incompletely immunized children. The incidence of otitis media caused by serotype 19F has remained steady. Overall healthcare utilization for otitis media has decreased, as has the incidence of recurrent otitis media in some populations and studies. [7, 23, 24, 25]
In June 2021, the pneumococcal conjugate vaccines PCV15 and PCV20 were licensed. Both contain the polysaccharides of PCV13; PCV15 additionally contains 2 additional serotypes, 22F and 33F, whereas PCV20 contains an additional seven (8, 10A, 11A, 12F, 15B, 22F, and 33F). These additional 7 included in PCV20 are responsible for approximately 30% or more of invasive pneumococcal disease cases in adults. [26] In October 2021, the CDC ACIP revised their pneumococcal vaccine guidelines to recommend the use of PCV20 or PCV15 in series with PPSV23 in all adults over the age of 65 or in age of 19-64 with certain underlying medical conditions. [27] As widespread uptake of these vaccines increases, population level changes in incidence of pneumococcal infection have not yet been extensively studied.
Pathophysiology
Capsule
The capsule is composed of polysaccharides that cover the cell wall, which is made up of peptidoglycan and teichoic acid, characterizing the classic gram positive structure; it acts as the principal antiphagocytic and protective element that prevents access of the leukocytes to the underlying cell wall elements. The capsular polysaccharides have served as means of serotyping and identifying these organisms. The Quellung reaction is the criterion standard method for pneumococcal capsular serotyping. More than 9 serotypes of S pneumoniae have been identified; serotypes 6, 14, 18, 19, and 23 are the most prevalent agents that cause infections. Serotyping provides important epidemiologic information, especially with the widespread use of vaccination, but rarely provides timely clinical information.
The virulence of each organism is determined in part by 2 distinct states: opaque and transparent colony types that influence the capacity to evade host defenses. The nasopharynx predominantly is colonized by the transparent phenotype. Conversely, the opaque type predominates in lung, CNS, and bloodstream infections; it has increased capsular polysaccharide and produces more biofilm. [28] In addition, in vitro and in vivo studies of clinical isolates have shown that pneumococci have the ability to obtain DNA from other pneumococci (or other bacteria) via transformation, allowing them to switch to serotypically distinct capsular type.
Adherence and Invasion
S pneumoniae is an extracellular bacterial pathogen that can adhere avidly to the respiratory epithelium and mucus. It exhibits different surface proteins that recognize and attach to human cells. Pneumococcal surface protein C (PspC) binds to the poly-Ig receptor on epithelial cells, pneumococcal surface antigen A (PsaA) binds to E-cadherin on epithelial cells, pneumococcal adhesion and virulence factor A (PavA) binds to fibronectin, and enolase (Eno) binds to plasminogen that may bridge binding to host cells. Phospho-cholines interact with the receptor for platelet-activating on activated epithelial cells. Capsule, pneumolysin, and the ABC transporter Ami have been implicated in adherence. [29] S pneumoniae produces biofilm after binding to host cells. Biofilm production is regulated by external factors, such as temperature.
Invasion is promoted by phospho-cholines. After interacting with the PAF receptor, it is inserted into the host cell via endocytosis, causing translocation of bacteria through the endothelium. This is particularly important for translocation over the blood-brain barrier during meningitis development. Bacteria surface coat is changed via gene expression to avoid host defenses and complete translocation. Invasion is also mediated by adhesins and pneumolysin; pneumolysin is a cytotoxin that induces apoptosis of epithelial cells by membrane pore formation, resulting in access to subendothelium. Intraalveolar replication of pneumococci, penetration into the interstitium, and dissemination into the bloodstream are among other functions of pneumolysin. [30]
Much of the clinical severity of pneumococcal disease results from the activation of the complement pathways and cytokine release, which induce a significant inflammatory response. S pneumoniae cell wall components, along with the pneumococcal capsule, activate the alternative complement pathway; antibodies to the cell wall polysaccharides activate the classic complement pathway. Cell wall proteins, autolysin, and DNA released from bacterial breakdown all contribute to the production of cytokines, inducing further inflammation.
Frequency
United States
Colonization
S pneumoniae remains an important pathogen in large part because of its ability to first colonize the nasopharynx efficiently. Studies performed in the United States prior to universal vaccination recommendations have shown average carriage rates of 40-50% in healthy children and 20-30% in healthy adults. Factors such as age, daycare attendance, composition of household, immune status, antibiotic use, and others obviously affect these numbers. [31, 32, 33] With the implementation of childhood vaccination with the heptavalent conjugate vaccine for S pneumoniae, the colonization rates have decreased in children receiving the vaccine and in adults and other children in their household because of the phenomenon of herd immunity.
Most individuals who are colonized with S pneumoniae carry only a single serotype at any given time; the duration of colonization varies and depends on specific serotype and host characteristics. Invasive disease usually is related to recent acquisition of a new serotype. However, in most healthy hosts, colonization is not associated with symptoms or disease but allows for the continued presence of S pneumoniae within the population, allowing for prolonged low-level transmission among contacts.
S pneumoniae infection is the most common cause of CAP, bacterial meningitis, bacteremia, and otitis media in the United States. There is a clear seasonality, with infections peaking in the fall and winter months. [34]
Noninvasive disease
Pneumococcal colonization allows for spread of organisms into the adjacent paranasal sinuses, middle ear, and/or tracheobronchial tree down to the lower respiratory tract. This spread results in specific clinical syndromes (sinusitis, otitis media, bronchitis, pneumonia) related to the noninvasive spread of the organisms.
Worldwide, the most common cause of death due to pneumococcal disease is pneumonia. In adults admitted to the hospital in the United States for pneumonia treatment, S pneumoniae remains the most common organism isolated. Until 2000, 100,000-135,000 patients were hospitalized for pneumonia proven to be caused by S pneumoniae infection in the United States annually. These numbers likely are a gross underestimate, as a definite cause is not determined in most cases of pneumonia treated each year. In addition, the actual rates are likely decreasing owing to implementation of pneumococcal conjugate vaccination. [35]
S pneumoniae infection is an important cause of bacterial co-infection in patients with influenza and can increase the morbidity and mortality in these patients. This has been emphasized recently by the increased number of cases of invasive pneumococcal disease seen in association with increased rates of hospitalizations for influenza during the 2009 H1N1 influenza A pandemic. [36] Postmortem lung specimens from patients who died of H1N1 influenza A from May to August of 2009 were examined for evidence of concomitant bacterial infection. Twenty-nine percent of the specimens showed evidence of bacterial co-infection, with almost half of these being S pneumoniae. [37]
S pneumoniae infection is estimated to cause over 6-7 million cases of otitis media annually in the United States. These numbers likely have decreased somewhat with the advent of universal vaccinations; however, S pneumoniae infection remains the most common cause of otitis media. [33, 38]
Invasive disease
Statistics regarding invasive pneumococcal disease in the United States are based on active surveillance using the Centers for Disease Control and Prevention (CDC) Active Bacterial Core Surveillance (ABC) system. Calculations for 2010 estimated 39,750 (12.9 cases per 100,000 population) cases of invasive disease nationally, with 4,000 (1.3 cases per 100,000 population) estimated deaths. (Comparable 2008 data showed 44,000 (14.5 cases per 100,000 population) episodes of invasive disease with 4,500 (1.5 cases per 100,000 population) deaths. [6]
Children younger than 5 years and adults older than 65 years are 2 identified age groups in whom rates of disease and death are increased. In 2010, rates of pneumococcal invasive disease in these groups were estimated to be 19 per 100,000 population and 36 per 100,000 population, respectively. This compares with rates of 20.2 and 40.4 in 2008, 21.8 and 39.2 in 2007, and 23.2 and 43.3 in 2002, respectively. More than half of deaths due to invasive pneumococcal disease occur in adults with specific risk factors (age, immunosuppression) for severe disease. Such risk factors are an indication for vaccination. [6, 39]
International
Despite the worldwide importance of disease due to S pneumoniae infection, very little information is available on the extent of pneumococcal disease in developing countries. A review of the available literature does show an increase in reports of incidence, prevalence, complications, and vaccine effects in many areas of Europe, Asia, and Australia.
Children
In developing countries, pneumococcus remains the most common and important disease-causing organism in infants. Although exact numbers are difficult to obtain, it is estimated that pneumococcal infections are responsible for more than 1 million of the 2.6 million annual deaths due to acute respiratory infection in children younger than 5 years. Case fatality rates associated with invasive disease vary widely but can approach and surpass 50% and are greatest in patients with meningitis; one quarter to more than one half of those who survive develop long-term sequelae of infection. [38, 40]
Estimates of pneumococcal disease in Gambian children show high rates of infection in the first year of life (≥500 per 100,000 children). [41] Latin American studies also show a particularly high risk in infants younger than 6 months, and children in southern India have higher rates of colonization at younger ages compared with US children, according to US clinical studies. Some particular populations, such as indigenous Australians and minority Israeli persons, also have disproportionately higher rates of disease, similar to the Native Alaskan and Native American populations in the United States, although determining the role of socioeconomic factors in the higher incidence of disease in these populations is difficult. [41]
In Europe, children younger than 2 years constitute the population most at risk for pneumococcal infection, with rates decreasing with age. The overall incidence of invasive disease is estimated to be somewhat lower in Europe (14 per 100,000 persons in Germany vs 35.8 per 100,000 persons in England vs 45.3 per 100,000 persons in Finland vs 90 per 100,000 persons in Spain vs 235 per 100,000 persons in the United States), although many have postulated that this may be due in part to the more liberal blood-culture collection practices in the American healthcare system. [41, 38]
Adults
Even fewer data are available on the worldwide incidence of pneumococcal disease in adults. As in the United States, the most common cause of CAP in Europe is S pneumoniae infection, affecting approximately 100 per 100,000 adults each year. Overall rates of febrile bacteremia and meningitis are also similar, (15–19 per 100,000 adults and 1–2 per 100,000 adults, respectively), with the risk for these diseases increased in elderly and infant populations. [42]
Because no population-based data on pneumococcal disease in adults in developing countries are available, estimates of disease burden are based on small clinical studies, vaccine trials, extrapolation from data in developed countries, and studies of persons at high risk for disease. The information gleaned from these sources suggests that the incidence of and mortality rates associated with pneumococcal disease are high, with HIV-positive populations exhibiting particularly high rates of infection. Further studies are greatly needed. [43, 38]
Mortality/Morbidity
Although exact rates are difficult to determine, the World Health Organization (WHO) estimates that, worldwide, 1.6 million deaths were caused by pneumococcal disease in 2005, with 700,000 to 1 million of these occurring in children younger than 5 years. [44] Even in patients in developed countries, invasive pneumococcal disease carries a high mortality rate—an average of 10-20% in adults with pneumococcal pneumonia, with much higher rates in those with risk factors for disease. [45, 46]
Race
In the United States, invasive pneumococcal disease is more common in Alaska Natives, Navajo and Apache Indians, and African Americans than in other ethnic groups. Some studies have shown this difference persists even when the results are controlled for socioeconomic factors, and the reasons for this discrepancy among certain populations are unclear. [32]
Sex
Most clinical studies of pneumococcal disease show a slight male predilection for disease; the reason for this is unclear.
Age
Children younger than 2 years carry the highest burden of S pneumoniae disease worldwide. In developed countries, the incidence is highest in those aged 6 months to 1 year, while, in developing countries, the disease is particularly common in children younger than 6 months.
Adults older than 55-65 years are the next most commonly affected age group worldwide.
Immunosuppressed persons of any age are at a higher risk for pneumococcal disease.
Epidemiology
S pneumoniae infections occur worldwide. Humans are the reservoir and transmit the infection via respiratory droplets or through autoinoculation. Although there are many serotypes that can cause infection, there are a few that cause the majority of infections. The communicability period is unknown, but spread can be affected by other factors such as viral respiratory infections. Infections are more common during the winter and early spring.
Prognosis
Pneumococcal conjunctivitis, otitis media, and sinusitis in developed countries where appropriate antibiotics are available usually carry an excellent prognosis; potential complications of these infections are listed above.
The prognosis of pneumococcal pneumonia depends largely on underlying factors, including age, immunosuppression, availability of antibiotics, and extent of lung involvement. It appears that most adults (mean age, 64.6 years) who survive invasive pneumococcal pneumonia lose a mean 9.9 years of longevity. [47]
The prognosis of pneumococcal meningitis is also related in part to host factors. Most studies have shown that morbidity rates in otherwise healthy US children with meningitis are usually less than 10%; however, neurological sequelae are common.
Patient Education
All parents should be advised of the recommendations for universal childhood immunization with the pneumococcal conjugate vaccine.
Patients with medical conditions that place them at an increased risk for serious or invasive S pneumoniae disease should be educated about their condition, the potential presenting signs and symptoms of pneumococcal infection, and the need to obtain medical care promptly upon any concern for possible infection. These patients should be educated about the benefits of the pneumococcal polysaccharide vaccine and should be encouraged to receive it.
-
Sputum Gram stain from a patient with a pneumococcal pneumonia. Note the numerous polymorphonuclear neutrophils and gram-positive, lancet-shaped diplococci. Courtesy of C. Sinave, MD, personal collection.
-
Lobar consolidation with pneumococcal pneumonia. Posteroanterior film. Courtesy of R. Duperval, MD.
-
Lobar consolidation with pneumococcal pneumonia. Lateral film. Courtesy of R. Duperval, MD.
-
Empyema caused by Streptococcus pneumoniae. Anteroposterior film. Courtesy of R. Duperval, MD.
-
Purpura due to pneumococcal sepsis in a 39-year-old man who underwent a splenectomy 20 years earlier. Courtesy of Thomas Herchline, MD, Wright State University, Dayton, Ohio.
Tables
- Table 1. Routine Vaccination With Pneumococcal Vaccines [88, 91, 92]
- Table 2. Vaccination of High-Risk Children Aged 2-18 Years With Pneumococcal Polyvalent Vaccine 23-Valent [93]
- Table 3. Vaccination of High-Risk Adults Aged 19 Years and Older With Pneumococcal Vaccines [91, 90]
- Table 4. Recommended Schedule for Doses of PCV13, PCV15, or PCV20 Including Catch-up Immunizations in Previously Unimmunized and Partially Immunized Children [92]
Population |
Vaccine |
|
Children aged 6 weeks through 5 years: 0.5 mL IM |
Pneumococcal conjugate vaccine 13-valent (Prevnar 13), 15-valent (Vaxneuvance), or 20-valent (Prevnar 20) Series of 4 doses at ages 2, 4, 6, and 12-15 months (catch-up schedule through age 5 y) |
|
Adults aged 65 years and older*†: 0.5 mL IM |
Adults who have not previously received a pneumococcal conjugate vaccine or whose previous immunization history is unknown should receive either PCV20 or PCV15 If PCV15 is used, follow with a dose of pneumococcal polyvalent vaccine 23-valent (PPSV23) after 1 year (or at least 8 weeks if immunocompromised) |
|
†Those who received PPSV23 before age 65 years for any indication should receive another dose of the vaccine at age 65 years or later if at least 5 years have passed since their previous dose. |
||
Pediatric Risk Group |
High-Risk Condition |
Chronic medical conditions |
Chronic heart disease (particularly cyanotic congenital heart disease and cardiac failure) Chronic lung disease (including asthma if treated with high-dose corticosteroids) Diabetes mellitus Cerebrospinal fluid leaks Cochlear implant Sickle cell disease and other hemoglobinopathies Anatomic or functional asplenia |
Hepatic disease |
Chronic liver disease, alcoholism |
Immunocompromising conditions |
HIV infection Chronic renal failure and nephrotic syndrome Immunosuppressive drugs or radiation therapy, malignant neoplasms, leukemias, lymphomas, Hodgkin disease, solid organ transplantation Congenital or acquired immunodeficiency |
Risk Group |
Condition |
Immunocompetent individuals |
Chronic heart disease* |
Chronic lung disease† |
|
Diabetes mellitus |
|
Cerebrospinal fluid leaks |
|
Cochlear implant |
|
Alcoholism |
|
Chronic liver disease, cirrhosis |
|
Functional or anatomic asplenia |
Sickle cell disease and other hemoglobinopathies |
Congenital or acquired asplenia |
|
Immunocompromised individuals |
Congenital or acquired immunodeficiency |
HIV infection |
|
Chronic renal failure |
|
Nephrotic syndrome |
|
Leukemia |
|
Lymphoma |
|
Hodgkin disease |
|
Generalized malignancy |
|
Iatrogenic immunosuppression‡ |
|
Solid organ transplant |
|
Multiple myeloma |
|
*Congestive heart failure and cardiomyopathies, excluding hypertension. †Including chronic obstructive pulmonary disease, emphysema, and asthma. ‡Diseases requiring treatment with immunosuppressive drugs, including long-term systemic corticosteroids and radiation therapy. |
|
Age at Examination (mo) |
Immunization History |
Recommended Regimen* |
2-6 |
0 doses |
3 doses, 2 mo apart; fourth dose at age 12-15 mo |
|
1 dose |
2 doses, 2 mo apart; fourth dose at age 12-15 mo |
|
2 doses |
1 dose, 2 mo after the most recent dose; fourth dose at age 12-15 mo |
7-11 |
0 doses |
2 doses, 2 mo apart; third dose at age 12 mo |
|
1 or 2 doses before age 7 mo |
1 dose at age 7-11 mo, with another dose at age 12-15 mo (≥2 mo later) |
12-23 |
0 doses |
2 doses, ≥2 mo apart |
|
1 dose at < 12 mo |
2 doses, ≥2 mo apart |
|
1 dose at ≥12 mo |
1 dose, ≥2 mo after the most recent dose |
|
2 or 3 doses at < 12 mo |
1 dose, ≥2 mo after the most recent dose |
24-71 |
|
|
Healthy children (24-59mo) |
Any incomplete schedule |
1 dose, ≥2 mo after the most recent dose† |
Children at high risk‡ (24-71 mo) |
Any incomplete schedule of < 3 doses |
2 doses, one ≥2 mo after the most recent dose and another dose ≥2 mo later |
|
Any incomplete schedule of 3 doses |
1 dose, ≥2 mo after the most recent dose |
*In children immunized before age 12 mo, the minimum interval between doses is 4 weeks. Doses administered at age 12 months or later should be administered at least 8 weeks apart. † Providers should administer a single dose to all healthy children aged 24-59 mo with any incomplete schedule. ‡Children with sickle cell disease, asplenia, chronic heart or lung disease, diabetes mellitus, CSF leak, cochlear implant, HIV infection, or another immunocompromising condition. PPV23 is also indicated (see below). |
||







