Overview
Vascular lesions of the head and neck encompass a wide range of different lesions. [1] Historically, these lesions have been poorly understood, and their nomenclature reflects this. Over the years, this nomenclature has evolved as progress has been made in our understanding of the histopathology, clinical behavior, treatment, and prognosis of these lesions.
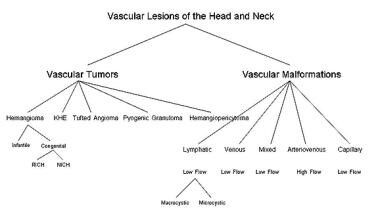
The first tangible steps toward better defining these lesions and tailoring the treatment were made in the early 1980s. In 1982, Mulliken and Glowacki developed the first binary system of diagnosis based on histologic characteristics, dividing these lesions into either hemangiomas or vascular malformations. [2] Since that time, our understanding of the histologic composition and clinical behavior of these lesions has continued to progress and additional subclassifications have been created (see the image below).
In addition, an international collaborative has been established to further refine the diagnosis and treatment of these lesions, the International Society for the Study of Vascular Anomalies (ISSVA). Treatment and prognosis vary considerably based on the correct diagnosis of the lesion, and new modalities are being described. Our understanding of the molecular biology and genetics of these lesions is evolving at a rapid pace and additional refinement of definitions and classifications is inevitable.
The purpose of this article is to examine some of the more common lesions within the current ISSVA classification system, focusing on the presentation and physiology of the specific lesions and their individualized treatment and prognosis. Current evaluation and treatment of these lesions in the pediatric population is often carried out in a multidisciplinary setting with a team of health care providers, including pediatric surgeons, head and neck surgeons, interventional radiologists, dermatologists, hematologists, and plastic surgeons. In this setting, a diagnosis is reached and a treatment plan created, streamlining a process that often requires multiple clinic visits and treatments over years and has historically been time consuming and inefficient for patients and their families.
Classification of Vascular Lesions of the Head and Neck
The current classification system adopted by the international medical community divides vascular lesions of the head and neck into vascular tumors and vascular malformations. This division most often occurs through careful examination of a lesion’s clinical appearance and biologic behavior. Radiographic investigation is often used in the diagnostic process, especially to aid in differentiating deep vascular tumors from deep vascular malformations and defining extent of the lesions and involvement of nearby structures. Histopathology via open or needle biopsy is rarely needed as an aid to diagnosis but should be performed in cases of lesions that behave in atypical, aggressive fashion.
Ultrasonography and magnetic resonance imaging (MRI) are the most commonly used radiographic techniques. On ultrasonography, infantile hemangiomas (the most common type of vascular tumor) appear as hypoechoic, heterogenous, well-defined lesions. They contain small cystic and sinusoidal elements. Doppler ultrasonography often reveals fast flow, while hemangiomas are in their proliferative phase. Ultrasonography of vascular malformations depends upon the type of lesion. Some exhibit small cystic spaces with minimal or no flow (microcystic lymphatic malformations). Others exhibit high flow through enlarged, ectatic vascular channels (arteriovenous malformations). Still other lesions, such as macrocystic lymphatic malformations or venous malformations, exhibit low or no flow within larger cystic spaces.
MRI is the mainstay for radiographic evaluation of deep vascular lesions of the head and neck and can aid in the differentiation of vascular tumor from vascular malformation. In addition, this modality allows differentiation of lesion from normal tissue, elucidates the flow pattern of the lesion (low vs high flow), and defines extent of the lesion. Proliferating hemangiomas and arteriovenous malformations have high-flow patterns on MRI and characteristic patterns of signal and enhancement, while venous and lymphatic malformations have low-flow patterns and their own characteristic patterns of signal and enhancement. [3]
Computed tomography (CT) scanning may be preferred for preoperative evaluation because most surgeons are comfortable with this modality. In addition, 3-dimensional techniques in CT angiography are gaining acceptance as a useful tool in diagnostic and preoperative evaluation of vascular lesions (see the image below). [4]

Vascular tumors include hemangiomas, kaposiform hemangioendothelioma (KHE), tufted angiomas (TA), pyogenic granulomas, hemangiopericytomas, and other rare lesions. These lesions have distinct histopathology and clinical behavior. The most common vascular tumor by far and the best understood is the hemangioma, of which the infantile subtype is the most common. Table 1 compares and contrasts characteristics of this most common vascular tumor with those of vascular malformations.
Vascular malformations are congenital malformations of capillaries, veins, lymphatic vessels, or arteries. They may also exist as a combination of different types of vessels (eg, the arteriovenous malformation). These malformations may further be divided into high-flow or low-flow lesions based on the vessel type. The lymphatic lesions may be further divided into macrocystic and microcystic based on the size of the cystic components within the lesion. Vascular malformations grow in proportion with the patient but can exhibit rapid growth or expansion following infection, trauma, or hormonal change (eg, puberty or pregnancy).
Table 1: Characteristics of Common Vascular Lesions (Open Table in a new window)
Vascular Tumor/Infantile Hemangioma |
Vascular Malformations |
|
|
Vascular Tumors
Hemangiomas
Hemangiomas represent the most common tumor in infants, occurring in up to 3-5% of all children. [5] Most hemangiomas affect the head and neck. They are more common in females by a ratio of 3:1 and usually manifest as an isolated, dark lesion of the skin within a few weeks to months of birth. These lesions are classified as infantile hemangiomas. While subtle at birth, they reveal themselves during proliferation. In addition to being more common in females, they are more common in whites and have up to 10% incidence in preterm infants. [6] One in 5 children affected develop more than one infantile hemangioma.
Other hemangiomas present at birth are already mature and do not proliferate. These are referred to as congenital hemangiomas and are divided into rapidly involuting congenital hemangiomas (RICHs) and noninvoluting congenital hemangiomas (NICHs). [7, 8] Most cases of RICH involute entirely by age 1 year. [9] NICHs do not decrease in size. Congenital hemangiomas account for approximately 3% of all hemangiomas. [10] Infantile hemangiomas are the focus of this section of the article.
Infantile hemangiomas are characterized by a phase of rapid proliferative growth characterized by increasing numbers of endothelial cells. This proliferative phase lasts up to one year and represents a clonal expansion. Hemangiomas in this phase have elevated levels of vascular endothelial growth factor (VEGF) and elevated populations of mast cells. Infantile hemangiomas are also positive for certain biologic markers, including glucose transporter isoform 1 (GLUT1). [7] Immunopositivity for GLUT1 may be used to separate infantile hemangiomas from congenital hemangiomas and vascular malformations, both of which are negative for this marker. [9]
The proliferative phase is followed by a prolonged phase of involution. Involution may last many years. A clinical pearl exists that complete involution occurs in 50% of lesions by age 5 years and in 70% of lesions by age 7 years. Involution leaves an area of expanded skin or mucosa (depending upon the location of the lesion) and loss of underlying normal subcutaneous fat and replacement with fibrofatty tissue. In addition, bone erosion or remodeling may have occurred due to the presence of the lesion.
Presentation and physical examination
Infantile hemangiomas usually present within the first few weeks to months of birth. The symptoms and signs are dependent upon the location and depth of the lesion. Superficial lesions that affect the skin manifest as raised, red lesions that are somewhat firm to the touch (see the first image below). Subcutaneous lesions tend to manifest as deeper masses with a blue hue and an unaffected overlying skin layer (see the second image below). These deeper lesions are more difficult to differentiate from vascular malformations and other masses and more often require radiographic imaging to aid in diagnosis. Hemangiomas may also contain both superficial and deep elements (see the third image below).



A study by Yanes et al looking at localized infantile hemangiomas of the lip indicated that these lesions do not occur at random locations but instead appear at sites that seem to correspond to known facial development models. [11]
Special mention should be made of subglottic hemangiomas. This particular location presents as increasing stridor in the infant. In a large review of these lesions, the mean age of symptom presentation was 2.7 months. [12] Flexible or rigid bronchoscopy is the customary diagnostic modality and reveals the presence of a submucosal swelling. The lesion may be unilateral to circumferential. Approximately 50% of patients with subglottic hemangiomas also have a cutaneous hemangioma. In addition, patients with hemangiomas in the "beard" distribution on the face have a higher incidence of subglottic hemangioma. [13]
Facial hemangiomas in a segmental distribution have been associated with posterior fossa malformations, hemangiomas, arterial anomalies, coarctation of the aorta, and eye abnormalities. This is known as PHACE syndrome. Other syndromes associated with hemangiomas include Maffucci syndrome (hemangiomas, enchondromas, and skeletal abnormalities) and blue rubber bleb nevus syndrome (multiple cutaneous hemangiomas and gastrointestinal hemangiomas). In children with 5 or more hemangiomas, the workup should include an abdominal ultrasonography to evaluate for visceral hemangiomas. [14]
Complications
The natural history of infantile hemangiomas is one of growth followed by involution. Complications occur at various points in this history and may be systemic or limited to the site of the lesion. Complications also occur as a result of intervention, both medical and surgical.
The aforementioned study by Yanes et al concerning infantile hemangiomas of the lip found poor outcomes associated with untreated segmental hemangiomas in comparison with localized lesions. Untreated localized hemangiomas of the upper lip or involving the vermilion border were also linked to poor outcomes, as were those of comparatively large size. [11]
Local complications
Local complications are many and are dependent largely upon the size and location of the lesion. Ulceration and infection occur commonly during the proliferative phase of superficial skin infantile hemangiomas, although one goal of early treatment is to avoid ulceration. [6, 14] The first-line treatment for both of these conditions is improved wound hygiene and topical antibiotic ointment. Laser therapy with the pulse dye laser may also be used early on for ulceration. Larger skin breakdown or infection may require intravenous antibiotics and/or systemic medical management (see the image below).

A multicenter, retrospective study by Gautam et al indicated that among infantile hemangiomas that lead to aggressive ulceration (AU), the clinical features tend to vary according to their anatomic location. Those in the head and neck region were usually localized and tended to be mixed (with both superficial and deep elements). In the diaper area, however, infantile hemangiomas with AU were typically segmental, and the superficial element tended to be thin. Segmental lesions, but with a thick superficial component, were found on the trunk and upper extremities. [15]
Scarring may occur as a natural consequence of hemangioma involution or as an outcome of ulceration. Small hemangiomas in nonvital locations may be managed with observation, but the deformity after involution may be unsightly and require surgical revision. Some lesions can cause significant aesthetic concerns that warrant treatment rather than observation. These lesions can be managed medically, surgically, or with laser treatment. These modalities may also be used in combination.
Periorbital hemangiomas may cause significant problems with vision, especially during the proliferative phase and slow involution (see the image below). During this period, binocular vision can be compromised with as little as one week of vision deprivation in the affected eye. [16] Deprivation amblyopia affects approximately 75% of children over the age of 1 year who were untreated. [17]

Airway compromise is a local complication of subglottic hemangiomas. Prior to propranolol, approximately one half of all subglottic hemangiomas require surgical intervention in addition to any medical management. [13] Untreated airway compromise may prove fatal. Tracheotomy, one of the surgical management techniques, has its own morbidity and mortality as well. Hemangiomas involving the parotid gland may also obstruct the airway, albeit at a higher level.
Systemic complications
Various systemic complications may occur with hemangiomas. Vascular tumors, such as kaposiform hemangioendotheliomas and tufted angiomas, may be associated with bleeding from a consumptive coagulopathy that results in thrombocytopenia, microangiopathic hemolytic anemia, and loss of clotting factors. [18] This clinical picture is referred to as Kasabach-Merritt phenomenon. [19] It is important to note that this phenomenon is not associated with infantile hemangiomas. The etiology of Kasabach-Merritt phenomenon is unknown, but platelet trapping occurs in enlarging vascular tumors and causes consumption of the coagulation factors. It is associated with a 20% mortality rate. These patients may require transfusion with blood or blood products to correct their coagulopathy should it become life threatening (see the images below). Therapy is directed at treating the tumor with agents such as corticosteroids, vincristine, or interferon. [20, 21]
 Deep vascular tumor with overlying skin discoloration in a 2-week-old infant with thrombocytopenia.
Deep vascular tumor with overlying skin discoloration in a 2-week-old infant with thrombocytopenia.
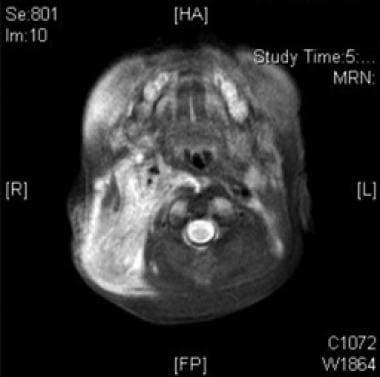 T2-weighted MRI of the infant in the image above demonstrating depth, infiltrative characteristics, and enhancement on T2-weighted imaging in this lesion, eventually proven to be kaposiform hemangioendothelioma (KHE).
T2-weighted MRI of the infant in the image above demonstrating depth, infiltrative characteristics, and enhancement on T2-weighted imaging in this lesion, eventually proven to be kaposiform hemangioendothelioma (KHE).
Congestive heart failure may occur in the setting of large and/or multiple hemangiomas located in the skin, subcutaneous tissues, or viscera. This complication is also associated with kaposiform hemangioendotheliomas and tufted angiomas. This complication may be due to years of wear and tear on the heart caused by moving blood rapidly through an additional large, high flow circuit. Large, deep, or visceral hemangiomas can be difficult to detect upon physical examination.
A high index of suspicion should be maintained for difficult to detect lesions and for heart failure in patients with multiple hemangiomas or with a KHE or TA. Because the liver is the most common site of involvement, [20] abdominal ultrasonography may prove diagnostic and is recommended in patients with KHE, TA, or multiple hemangiomas as a screening tool. Patients with congestive heart failure may require intensive medical management.
Treatment
Because hemangiomas may occur anywhere, as single or multiple lesions, as superficial or deep visceral lesions, treatment varies considerably in method and timing. The physician should remember that observation may be a suitable for certain lesions. Some lesions are better dealt with once they have involuted, or they may turn out to require no pharmacotherapy or surgery whatsoever. Treatment is indicated when functional or cosmetic complications arise (or are predicted to arise) that are worse than the side effects of intervention. Lesion size, location, patient age, and phase of the lesion (proliferative, involuting, mature) also influence the method and timing of intervention.
Pharmacotherapy
The biggest advance in pharmacotherapy for the treatment of infantile hemangiomas has been propranolol. In 2008, it was first described that these lesions responded to the medication, and numerous studies since then have confirmed this. [22, 23] Propranolol has now become a mainstay of treatment for hemangiomas. The dosing and length of treatment can vary, although many patients are treated with 2 mg/kg/day divided into 2-3 doses for up to age 1 year, as this is the proliferative phase. In March 2014, a pediatric formulation of propranolol hydrochloride (Hemangeol) was approved by the US Food and Drug Administration for the treatment of proliferating infantile hemangioma needing systemic therapy. [24]
One benefit of propranolol over systemic steroids is that the effects can be lasting after discontinuation of propranolol, while with steroids the lesion can quickly proliferate again after discontinuing treatment if still in the proliferative phase. The exact mechanism of how the beta-blocker causes regression in infantile hemangiomas has not been proven, but it may act by down-regulating factors that enhance endothelial growth and/or by triggering apoptosis of endothelial cells within the lesion. Studies have shown greater than 80% response, although a retrospective study by Wu et al indicated that propranolol demonstrates better short-term efficacy in the treatment of infantile hemangiomas (mean follow-up time = 6.2 months) when the lesions are less than 1.2 cm thick. [6, 25, 26] The images below show before and after treatment with propranolol.

 The same large hemangioma of infancy as in the previous image after just 1 week of propranolol treatment.
The same large hemangioma of infancy as in the previous image after just 1 week of propranolol treatment.
Adverse effects of propranolol include bradycardia, hypotension, hypoglycemia, and bronchospasm. Many institutions now have interdisciplinary teams for the treatment of vascular malformations and include a cardiologist to help with management of propranolol treatment. [23] Recent guidelines recommended the initiation of propranolol treatment in an inpatient setting for patients younger than 8 weeks or with any comorbidities, but outpatient treatment for those older than 8 weeks and otherwise healthy. [27]
Prior to propranolol, corticosteroids were the first-line medical therapeutic intervention for hemangiomas in the proliferative and involution phases. Steroids do continue to play an integral role in the treatment but are often not the first-line treatment anymore. Results have been published supporting the use of topical steroids in infantile hemangioma. [28] Steroids may also be given intralesionally, especially in the case of localized lesions. For instance, small yet problematic subglottic hemangiomas may be managed with repeated submucosal injections. [29] This method is often combined with other endoscopic interventions and may require postoperative intubation secondary to swelling after injection.
Oral steroid therapy is another common medical intervention. Doses used are usually in the range of 2-3 mg/kg/day prednisone or equivalent dose of another steroid. Results should be visible as a change in color and a decrease in size. Results should also be palpable as a softening of the lesion within 1-2 weeks. Oral steroids need to be tapered off after weeks of treatment. Hemangiomas in the proliferative phase that respond to steroids may increase in size again once the steroids are tapered. Approximately 20-30% of hemangiomas fail to respond. [30]
The mechanism of steroid therapy in hemangioma treatment is unknown. Steroids also have a long list of potential side effects, especially when used for the lengths of time often required by the hemangioma. Patients treated with systemic oral steroids should be monitored for hypertension, weight loss or gain, growth retardation, and suppression of the adrenal axis. Adrenal suppression and failure to thrive have also been reported following local injection of steroids. [31] In addition, the possible development of gastritis necessitates prophylactic histamine-2 receptor blocker or proton pump inhibitor therapy. Immune suppression may occur as well, and some have suggested that patients not receive live virus vaccine and potentially receive antibiotic prophylaxis against pneumocystis carinii and atypical mycobacterium.
Interferon has an antiangiogenic effect and decreases the rate of endothelial proliferation. It was historically used in the treatment of aggressive hemangiomas, often as an adjunct to steroids. Response often requires weeks to months of therapy. [32] The long list of side effects for this medication includes spastic diplegia, a potentially irreversible neurological condition. [33] For this reason, other adjuncts are often used in place of interferon.
Other less commonly used treatments include embolization and vincristine. [21] Embolization has also been described in the treatment of vascular tumors that are causing Kasabach-Merritt phenomenon. [34] Vincristine, a cytotoxic alkaloid often used as a chemotherapeutic agent, has an antiangiogenic effect and has also been described in the treatment of lesions associated with Kasabach-Merritt phenomenon and those compressing vital structures. [35, 36]
A retrospective study by Wang et al indicated that vincristine is a safe and effective treatment for steroid-resistant kaposiform hemangioendothelioma (KHE) with Kasabach-Merritt phenomenon. Among the study’s 37 patients, complete remission occurred in 26 lesions. [37]
Laser therapy
Multiple lasers have been employed in the treatment of infantile hemangiomas. The pulsed-dye laser (PDL) is a commonly used laser in the treatment of vascular lesions; however, controversy exists regarding its use in hemangiomas. [38] Evidence exists supporting the use of the PDL in ulcerated lesions. [39, 40] The carbon dioxide (CO2) laser has been used extensively in the treatment of subglottic hemangiomas. In a large review of these particular lesions, CO2 laser was the most extensively used modality and had a complication rate of about 12%, most notably subglottic stenosis. [12] Diode lasers such as the Nd:YAG have also been used.
Surgical management
Surgical excision of infantile hemangioma has multiple indications, as follows [41] :
-
Threat to life or function (airway, vision, mobility, limb)
-
Complicated course (ulceration, hemorrhage, infection, heart failure)
-
Failure of pharmacotherapy
-
Removal of fibrofatty residuum
-
Cosmetic revision of scars after lesion involution
-
Atypical growth or prolonged course
-
Emotional burden on the child or family without undue surgical risk
Not all lesions fitting these criteria require removal, nor will all lesions excised meet these criteria perfectly. In addition, the timing of surgery is often controversial. Parents may wish to have a lesion excised that the treating physician believes will involute completely or at least be easier to excise at a later date. The risks of the procedure must be weighed against the predicted benefits of a more conservative management.
Treatment of the subglottic hemangioma
The treatment of these unique lesions deserves special mention, principally because of the number of options and the amount of controversy present. Treatment includes such varied options as observation, tracheotomy, and waiting for involution, medical management, endoscopic techniques (laser, microdebrider, steroid injection), and open excision. Smaller lesions that are relatively asymptomatic may be observed or treated medically with propranolol or oral steroids. Symptomatic lesions are often treated with both propranolol and steroids, if not endoscopic laser treatment.
These patients are often left intubated for several days to allow for swelling to improve, and these procedures often need to be repeated. Larger lesions that are significantly obstructing the airway may require tracheotomy. Certain centers have treated these larger lesions with open surgical excision, often with excellent outcomes and the added benefit of potentially shortening the treatment to one procedure (see the images below). [42, 43] Again, propranolol has altered management even with larger airway lesions, and it is likely that less patients will require open surgical therapy. Attempts to compare the outcomes of these modalities are complicated by the selection bias used to choose the modality at certain centers and the nonstandardized methods used by individual surgeons. Readers are referred to the excellent review by Bitar and others. [12]


Vascular Malformations
Vascular malformations are congenital malformations of capillaries, veins, lymphatics, or arteries, alone or in combination. These lesions are not characterized by endothelial proliferation or involution. Instead, they are characterized by proportional growth and possible rapid growth in the setting of trauma, infection, or hormonal change. Vascular malformations are congenital, meaning that they are present at birth. Most are diagnosed during infancy, although some are noticed later in childhood, as in the case of a lymphatic malformation that presents after viral upper respiratory infection. These lesions may also be distinguished by the rate of flow and size of lymphatic cystic components, as seen in the image below.
Diagnosis is often accomplished by a thorough history and physical examination. The age at which the lesion was noticed (congenital), its lack of proliferative growth, subtle color distinction from normal tissue, and compressibility all hint at the diagnosis of vascular malformation. If the lesion has grown rapidly, investigating precipitating events such as upper respiratory tract illness or local trauma is useful. Palpating for a thrill or pulsation and to auscultate for a bruit is also useful.
After history and physical examination, radiological investigation is often the next step in distinguishing vascular malformations from vascular tumors and in mapping the extent of the lesion.
Capillary malformations
Capillary malformations are congenital anomalies of capillary and/or small vein development. They most commonly occur in the papillary and superficial reticular dermis. Capillary malformations are low-flow lesions. They occur in 0.3% of newborns and should be distinguished from the more common macular stains of infancy that fade over time. Nevus flammeus, also called stork bites or angel kisses, are a collection of capillaries near the surface of the skin often found near the nape of the neck or on the face. They occur in up to a third of infants and usually resolve without any intervention. [14]
Research indicates that capillary malformations arise from an R183Q mutation in the GNAQ gene, with this anomaly being found in 90% of such malformations occurring nonsyndromically and in Sturge-Weber syndrome. [44]
Presentation and physical examination
Capillary malformations of the head and neck region usually present at birth as a pink macular lesion and can occur in the distribution of the trigeminal nerve. These may fade or darken as the child ages. Certain capillary malformations manifest at birth that do not fade are known as port wine stains. These are dark red, raised lesions that persist throughout the individual’s life. Many capillary malformations are slightly rubbery upon palpation.
Complications
Sturge-Weber syndrome deserves special mention in any discussion of capillary malformations. Port wine stains in the distribution of the first division (V1) or second division (V2) of the trigeminal nerve are a characteristic of this rare autosomal dominant condition. Certain subtypes of this condition are associated with central nervous system vascular lesions (such as leptomeningeal capillary malformations, venous malformations, or AVMs) as well as with lesions of the eye, including glaucoma. [20] These children may have seizures and learning or behavior difficulties. Patients with capillary malformations of the face warrant an investigation for Sturge-Weber syndrome, including imaging of the brain and ophthalmologic investigation. Patients suspected of having Sturge-Weber syndrome should be referred to both a neurologist and ophthalmologist. Klippel-Trenaunay-Weber syndrome also is associated with port wine stains, venous malformations, and hypertrophy of the associated limb.
Several other genetic conditions are associated with capillary malformations, including hereditary hemorrhagic telangiectasia (HHT) and ataxia-telangiectasia. HHT is associated with mucosal and visceral lesions that bleed easily. Ataxia-telangiectasia is associated with central nervous system dysfunction, cutaneous telangiectasia, and immune compromise. Despite these genetic conditions and their unusual manifestations, the most common complications of capillary malformations are cosmetic.
Treatment
Laser therapy is the most common intervention for the routine capillary malformation. Of the available laser, the PDL is the most widely used. The PDL’s wavelength allows the energy to be absorbed by hemoglobin within the lesion rather than overlying and surrounding normal tissue and has a 50-70% response rate. [45] The Nd:YAG laser has found application in the treatment of the mucosal lesions of HHT.
Venous malformations
Venous malformations are present in 1-4% of the population. [20] They may be in the epidermis/dermis or within muscle or bone. Histologically, these lesions are composed of ectatic, poorly organized venous channels that have normal endothelium and lack the normal smooth muscle architecture that usually surrounds veins. Instead, muscle cells are arranged in unorganized fashion. [45] Venous malformations are low-flow lesions.
Presentation
Venous malformations are present at birth, although not all are clinically evident. They are the most common type of vascular malformation. Most are asymptomatic swellings that have a blueish hue, are compressible and not pulsatile, and have no palpable thrill or audible bruit. Some lesions have palpable phleboliths within them, a diagnostic hallmark of the venous malformation. If located in the head and neck, some lesions increase in size with compression of the ipsilateral jugular vein. Valsalva maneuver may also increase the size of the lesion, as will any high cardiac output state.
The most common locations for involvement in the head and neck are the masseter muscle, skin, lips/oral mucosa, and mandible. Mandibular lesions may present with loosening of teeth or bleeding. Lesions may also occur in the orbit, causing exophthalmos and vision changes. The images below show striking venous malformation of the head and neck that is after multiple resections and embolizations.

 Intraoral component of venous malformation in the same patient in the image above.
Intraoral component of venous malformation in the same patient in the image above.
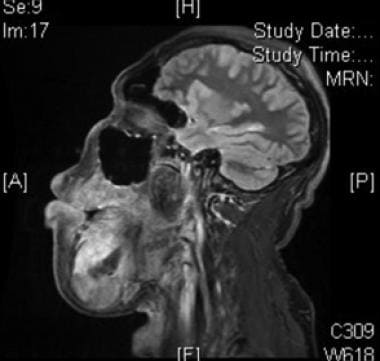 Sagittal fat-suppressed T1 postcontrast MRI of venous malformation in the same patient in the 2 images above.
Sagittal fat-suppressed T1 postcontrast MRI of venous malformation in the same patient in the 2 images above.
Radiological evaluation is used to confirm the diagnosis of venous malformation and to help distinguish between these lesions and other vascular anomalies. Phleboliths are often visible on plain film and are likely the result of sluggish, abnormal flow through the lesion’s ectatic channels. [20] MRI reveals a hyperintense lesion on T2, which enhances with contrast on T1 in the vascular channels (as opposed to lymphatic malformations, see below) and has flow voids where phleboliths are located. [20, 46]
Complications
Venous malformations can cause a multitude of complications. Even small lesions may be painful. This is likely secondary to phlebolith formation. Lesions may also become infected, as can any clots that form in the abnormal vascular channels. Cosmetic problems can occur with large lesions that cause contour abnormalities of the soft tissues and bony skeleton of the face and neck.
Treatment
If the lesion is small and symptoms are absent or minimal, reassurance and observation are likely the best treatment. For lesions that warrant a higher degree of intervention, there are essentially 2 modalities, both of which are frequently used in combination: sclerotherapy and surgical excision.
Surgical excision of limited lesions is sometimes an excellent choice for initial treatment. Sclerotherapy may also be used as a single modality for small lesions. Unfortunately, many venous malformations of the head and neck infiltrate many tissue planes and are intimately associated with vital nerves and vessels. For this reason, surgical excision is often used as a debulking procedure after sclerotherapy.
To date no prospective trials have compared the various sclerosing agents. The most commonly used sclerosing agents for venous malformations are ethanol and sodium tetradecyl sulfate STS), although doxycycline is another agent used. [20, 47, 48] These agents are injected directly into the lesions, often with ultrasonographic, fluoroscopic, or MRI guidance and often in multiple settings because the malformations are large and have a propensity to recanalize.
Reports have been published on the safe and effective use of ethanol for the treatment of venous malformations. [47, 49] Ethanol is inexpensive and easy to administer. However, it is painful and requires general anesthesia. To enhance exposure of the lesion’s endothelium to the ethanol, limitation of venous outflow may be required (manual or rubber-band compression). Complications of ethanol sclerotherapy include pain, skin necrosis, transient neuropathy, bleeding, renal toxicity, cardiac arrest, and anaphylaxis. [49, 50] STS has a lower incidence of serious side effects when compared with ethanol but may be less effective as well. [50] Bleomycin is a newer agent that has been used for sclerotherapy.
Lymphatic malformations
As with other vascular malformations, lymphatic malformations are present at birth and lined by nonproliferating endothelium. More than 50% are recognized at birth and 90% by age 2 years. [14] They may occur anywhere in the body, although the head and neck region is most commonly affected. Lymphatic malformations are low-flow lesions and may exist as combinations of lymphatic and venous vessels, in which case they are termed venous-lymphatic malformations. Older literature refers to lymphatic malformations by names such as "cystic hygroma" and "lymphangioma." These terms should be abandoned because they imply tumor characteristics that these lesions do not possess. Lymphatic malformations usually grow commensurate with the patient but may rapidly expand secondary to infection, trauma, or hormonal disturbance.
Lymphatic malformations can be macrocystic, microcystic, or a combination. Microcystic lesions are composed of small cystic spaces less than 1 cm in diameter. Although they may present anywhere in the head and neck, microcystic lesions most commonly occur superior to the mylohyoid muscle in the oral cavity or oropharynx. They may also be present in the parotid and preepiglottic space. Macrocystic lesions are composed of larger cystic spaces and usually occur lower in the neck. [20] Whether microcystic or macrocystic, lymphatic malformations contain eosinophilic and proteinaceous fluid. The vessels are surrounded by abnormal collections of smooth and striated muscle. [20]
Presentation
Microcystic lymphatic malformations are composed of clear vesicles within the subcutaneous tissue and muscles. These small cystic structures coalesce to form somewhat firm lesions that infiltrate the surrounding normal tissues. These lesions most commonly occur superior to the mylohyoid muscle, in the oral cavity for example (see the image below). Macrocystic lesions are more often softer and more easily compressed. They commonly appear underneath blueish discolored skin and as translucent swellings when exposed surgically. [20] They are usually less infiltrative into surrounding normal tissue. All patients with lymphatic malformations of the head and neck should have imaging of the lesion and, should the lesion be present in the lower neck, of the chest as well to evaluate for thoracic involvement.

Large lymphatic malformations are often noticed in utero during routine ultrasonography. These lesions may be further defined by MRI, usually in the second trimester. Microcystic lesions appear as isodense and infiltrative lesions. Macrocystic lesions have ringlike margin enhancement and are sharply demarcated from the surrounding normal tissue. [20] With large lesions noticed in utero, airway compromise is of concern. These patients and their mothers may require nonroutine delivery location and method. Ex utero intrapartum treatment (EXIT procedure) may be necessary to control the patient’s airway during delivery. In this procedure, the patient is partially delivered from the uterus and maintained on placental circulation until definitive airway management is achieved. Interventions range from simple laryngoscopy and intubation, flexible or rigid bronchoscopy and intubation, to a surgical airway (tracheotomy).
A staging system for lymphatic malformations has been proposed based on location above or below the hyoid bone and whether the lesion is unilateral or bilateral. Unilateral infrahyoid lesions have the best outcomes with surgical intervention. [51]
Complications
Many possible complications may arise from lymphatic malformations, including airway compromise, infection, and disfigurement. Airway compromise may occur at birth secondary to obstruction from the mass effect of the lesion. In addition, airway compromise may occur when the lesion rapidly enlarges, as occurs in the setting of infection, trauma, or hormonal disturbance. Large lesions may cause secondary disturbances in bone and soft tissue growth, leading to disfigurement.
Complications may also occur secondary to treatment. Surgical excision is associated with scar tissue both internally and within the skin, in addition to placing often intimately involved vessels and nerves at risk. Sclerotherapy is associated with post-treatment swelling, which may compromise the airway and/or swallowing, requiring intervention. For this reason (and because significant pain is associated with the procedure), sclerotherapy is often performed in the hospital under general anesthesia, and patients are usually observed for swelling and respiratory compromise for 24 hours.
Treatment
The ideal treatment strategy for lymphatic malformations depends upon numerous factors, including the location of the lesion and its extent of infiltration into normal tissues, whether it is microcystic or macrocystic, and the complications encountered or predicted for that particular lesion. As with vascular malformations, essentially 2 major treatment strategies exist other than observation: surgical excision and sclerotherapy.
Surgical excision is an ideal treatment for those lesions that are amenable. Previously untreated macrocystic lesions are the best candidates for this approach. They are often lower in the neck (below the mylohyoid muscle), less infiltrative, and easier to follow through tissue planes surgically when compared with their microcystic counterparts. However, they may be intimately involved with neurovascular structures within the neck (see the images below).
 Axial CT with contrast of macrocystic lymphatic malformation inferior to mylohyoid muscle.
Axial CT with contrast of macrocystic lymphatic malformation inferior to mylohyoid muscle.
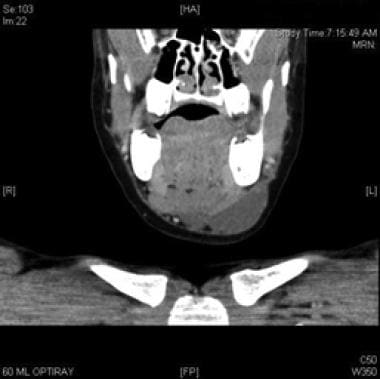 Coronal CT scan with contrast of macrocystic lymphatic malformation inferior to mylohyoid muscle.
Coronal CT scan with contrast of macrocystic lymphatic malformation inferior to mylohyoid muscle.
 Sagittal CT with contrast of macrocystic lymphatic malformation inferior to mylohyoid muscle.
Sagittal CT with contrast of macrocystic lymphatic malformation inferior to mylohyoid muscle.
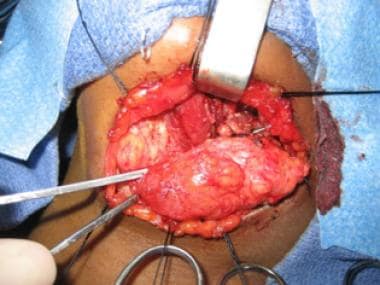 Intraoperative view of macrocystic lymphatic malformation. The digastric muscle is visible in the center of the wound.
Intraoperative view of macrocystic lymphatic malformation. The digastric muscle is visible in the center of the wound.

Surgical excision is also the treatment of choice for microcystic lesions, because these are more challenging if not impossible to treat with sclerotherapy. In these cases, limited excision is often the rule because the lesions are more infiltrative, lack distinct planes separating them from normal tissue, and are often too involved with vital structures to permit complete excision. [20] CO2 and Nd:YAG lasers have been used to facilitate limited excision of these difficult lesions.
Sclerotherapy is an excellent treatment choice for macrocystic lesions, the removal of which jeopardizes vital structures, or for patients who are poor surgical candidates. Although not "curative" in that the lesion is not removed, most patients achieve a 50% or greater reduction in the size of the lesion. [52] In a large review of the literature on sclerotherapy, Acevedo et al found that 87.5% of patients had some amount of positive response to sclerotherapy and only 12.5% went on to require subsequent surgery. [52] These authors conclude that sclerotherapy may be an appropriate first-line therapy for macrocystic lymphatic malformations. Many lesions require only one treatment session, although it is not rare to repeat the session should the initial result be unsatisfactory.
Numerous agents have been and are being used for sclerotherapy including ethanol, STS, bleomycin, and OK-432 (a lyophilized strain of group A Streptococcus pyogenes incubated with benzylpenicillin). OK-432 and bleomycin are the most commonly used agents. [52] OK-432 has been shown to stay within the lymphatic channels of the lesion and is associated with less fibrosis in the surrounding normal tissues when compared with other agents. [53] In addition, OK-432 is associated with a more favorable side effect profile than bleomycin. It’s most common side effects are pyrexia, local pain, and erythema, although major complications such as edema and airway compromise are possible. [52] Bleomycin is associated with pulmonary toxicity in addition to swelling.
Ultimately, the choice of interventions depends upon the particular lesion and the preferences of the physician and parents, in addition to the particular skill set of the treating physician. In patients with minimal functional impairment, observation alone may suffice, as some reports indicate complete regression with no intervention. [54]
Arteriovenous malformations
Arteriovenous malformations (AVMs) are high-flow lesions that allow shunting of blood from the arterial system directly into the venous system. It is thought that they are residua from failure of primitive vascular communications to obliterate. They are rare compared with other vascular lesions. They are most commonly found in the head and neck region, especially intracranially, and are the most dangerous of all vascular lesions. [3] Although they do not proliferate as hemangiomas do, AVMs may grow, usually secondary to the development of collateral channels for blood flow. In addition, these lesions share the ability with other vascular malformations to expand rapidly with infection, trauma, or hormonal disturbance.
Histologically, the artery walls contain disorganized smooth muscle. The veins undergo progressive hypertrophy, intimal thickening, and sclerosis, likely as a reaction to the volume and rate of blood flow they are required to accommodate. [20]
Presentation
AVMs are often noted at birth. In infancy, they are almost universally asymptomatic and are frequently confused for a hemangioma or capillary malformation. They eventually manifest as subcutaneous or submucosal swellings that are warm to the touch, have a palpable thrill, and an audible bruit. [3] This usually occurs in late childhood, adolescence or early adulthood, possibly secondary to hormonal changes. When the lesion expands, blood is shunted away from the skin and bones, possibly leading to skin ulceration and bone necrosis. [20]
The diagnosis of these lesions is based on the history of physical examination, supported by ultrasonography and radiography. Doppler ultrasonography likely reveals ectatic vessels with high flow. MRI and MRA are often used to confirm clinical suspicion and define the extent of the lesion. MRI reveals a high-flow lesion with flow voids and diffuse enhancement with contrast. MRA reveals the tangled, ectatic nature of the lesion’s vasculature and the main feeding vessels from the normal circulation.
Complications
AVMs can cause pain, expansion, and disfigurement, ulceration, life-threatening bleeding, cardiac hypertrophy, and cardiac failure secondary to sustained high cardiac output. [3] Excessive bleeding and its associated morbidities and potential mortality may occur during resection of these lesions. Stroke is another well-known complication of intracranial AVM.
Treatment
Small, asymptomatic lesions are best observed. Surgical excision has been used, most often following attempts to embolize the lesion. In fact, intraarterial embolization followed by surgical excision is the only "curative" treatment modality. However, these lesions are often intimately involved with vital structures and the facial skeleton, making their complete surgical removal impractical. [3] Embolization usually precedes surgery by 1-2 days and is designed to decrease blood loss and facilitate surgery, not shrink the mass. [20]
Embolization may be used as a single modality in the palliation of patients whose lesions are not resectable without unacceptable complications. Surgical ligation of feeding vessels has little role. This is thought to lead to rapid recruitment of other vessels and to obliterate a potential route for embolization. [20]
Future Directions
Modern medicine has clearly made a great deal of progress in the diagnosis and management of vascular lesions. The treating physician is often a member of a multidisciplinary team and has at his or her fingertips treatment modalities that have resulted from genetic research, modern imaging, and evidence-based study. Nevertheless, a great deal remains to be done, especially in the case of those lesions that are difficult to treat medically and that are associated with surgical comorbidities, as in the case of subglottic hemangioma.
-
Classification of vascular lesions of the head and neck.
-
Three-dimensional CT angiogram of a submental vascular lesion (arrow).
-
Superficial infantile hemangioma.
-
Deep infantile hemangioma.
-
Combined superficial and deep infantile hemangioma.
-
Ulceration of infantile hemangioma.
-
Periorbital infantile hemangioma that is compromising vision.
-
Deep vascular tumor with overlying skin discoloration in a 2-week-old infant with thrombocytopenia.
-
T2-weighted MRI of the infant in the image above demonstrating depth, infiltrative characteristics, and enhancement on T2-weighted imaging in this lesion, eventually proven to be kaposiform hemangioendothelioma (KHE).
-
Subglottic hemangioma prior to open excision.
-
Subglottic hemangioma after open excision.
-
Venous malformation of the head and neck in an adolescent.
-
Intraoral component of venous malformation in the same patient in the image above.
-
Sagittal fat-suppressed T1 postcontrast MRI of venous malformation in the same patient in the 2 images above.
-
Microcystic lymphatic malformation of the tongue and floor of mouth.
-
Axial CT with contrast of macrocystic lymphatic malformation inferior to mylohyoid muscle.
-
Coronal CT scan with contrast of macrocystic lymphatic malformation inferior to mylohyoid muscle.
-
Sagittal CT with contrast of macrocystic lymphatic malformation inferior to mylohyoid muscle.
-
Intraoperative view of macrocystic lymphatic malformation. The digastric muscle is visible in the center of the wound.
-
Intraoperative view of macrocystic lymphatic malformation.
-
Large hemangioma of infancy before propranolol treatment.
-
The same large hemangioma of infancy as in the previous image after just 1 week of propranolol treatment.
Tables
Vascular Tumor/Infantile Hemangioma |
Vascular Malformations |
|
|





