Practice Essentials
Z-plasty is a common plastic surgery technique that at its core trades a shorter, simpler scar for a longer, more complex one. When the skin is undermined, 2 triangular flaps are created. Transposition of these triangles redistributes tension on the wound and changes central limb direction. The new scar elongates based not only on the character and elasticity of the surrounding skin but also on the angle size used in the Z-plasty.
The decision to utilize a Z-plasty must take into account the increased length and complexity of the scar, and this must be a worthwhile tradeoff in improving an existing scar.
Z-plasty is one of many techniques for scar revision and camouflage. It produces a type of transposition flap that incorporates qualities of advancement and rotation flaps into its design. Whether used alone or in conjunction with other scar-camouflage techniques, Z-plasty is a versatile maneuver that, when mastered, provides aesthetically pleasing results. [1, 2]
In 1856, Denonvilliers first described the Z-plasty technique as a surgical treatment for lower lid ectropion. The first reference to this technique in American literature was in 1913, by McCurdy, as treatment for contracture at the oral commissure. Limberg, in 1929, provided a more detailed geometric description. Numerical data showing optimal angles and length relationships of Z-plasty limbs are credited to Davis (1946).
The image below depicts a Z-plasty.
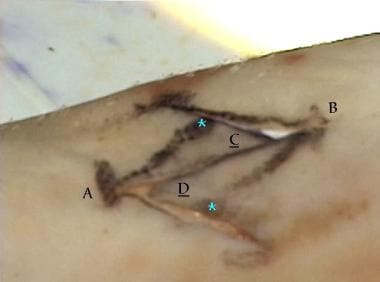 The original scar is A-B. The limbs of the Z-plasty form 2 triangles with 45° angles at apices C and D.
The original scar is A-B. The limbs of the Z-plasty form 2 triangles with 45° angles at apices C and D.
Indications
Z-plasty is an especially useful technique when dealing with a scar that crosses relaxed skin tension lines. Simple redirection of the central limb into these lines can provide adequate camouflage. The redistribution of tension on the wound provided by Z-plasty can be very helpful when dealing with a contracted scar or with a scar near aesthetic units, such as the medial canthus or oral commissure.
Z-plasty is an effective method of wound irregularization. Since straight-line scars draw attention easily, multiple Z-plasties can break up the scar into smaller units, making the scar less noticeable.
Other uses of Z-plasty are as follows:
-
Limiting/preventing contracture of linear scars, especially when they cross the border of a facial aesthetic unit (eg, vermillion border) or when scars cross a concave surface (eg, the medial canthus)
-
Changing scar length (eg, scar contracture of lip, eyelid, or neck)
-
Changing scar vector (eg, repositioning a scar across the nasolabial fold)
-
Repositioning malposed tissues (useful for "trapdoor" or "pin-cushion" defects)
-
Effacing web/release contracture (similar to first listed use)
-
Closing cutaneous defects (eg, large oval defects, pharyngocutaneous fistulae)
-
Correcting stenosis (eg, tracheostoma, nares, external auditory canal) using single or multiple Z-plasties [3]
-
Transposing healthy tissue to close a fistula (eg, tracheostoma closure after irradiation)
A study by Park et al indicated that fingertip injuries can effectively be repaired using a unipedicled volar rotational advancement flap with a large Z-plasty. The study encompassed 112 fingers that had sustained injury or finger pulp avulsion. The repair technique involved making a longitudinal incision along the injured digit’s lateral border and elevating a large neurovascular volar flap “just above the pulleys and flexor tendon sheath.” Tension was released by employing a large Z-plasty at the metacarpophalangeal joint or interphalangeal joint crease. The investigators found that no flap necrosis, postoperative contracture deformities, joint stiffness, long-term paresthesia, or hypersensitivity resulted, and determined that “average static two-point discrimination was 5.2 mm.” Two patients demonstrated partial wound dehiscence, and hypertrophic scarring developed in one patient at the linear incision site. [4]
A study by Scheller et al indicated that vertical Z-plasty is effective in the secondary correction of whistle deformities in patients who have undergone surgery for unilateral or bilateral cleft lip/palate. The procedure in the report involved the use of two triangular transposition vermilion flaps, with parts of the orbicularis oris muscle employed in the operation. All patients achieved a significant reduction in the defect score (DS), with the outcomes being rated as acceptable (DS >30), good (DS 10-30), and very good (DS 0-10) in 6, 5, and 23 patients, respectively. [5]
The Furlow double-opposing Z-plasty has gained wide acceptance since its introduction in 1978 as a means of cleft palate repair. The technique lengthens the soft palate and restores the velum anatomically and functionally. In a retrospective study, Lerner et al reported that as an alternative in patients in whom two Z-plasties are contraindicated, a cleft palate can be repaired with a single Z-plasty technique, with this surgery lengthening the soft palate and total palate by 33% and 10%, respectively. [6, 7]
A study by Ahti et al indicated that in patients with isolated cleft palate who suffer velopharyngeal insufficiency after repair, Z-plasty can be safely and effectively used in palatal re-repair. This strategy had an 81% overall success rate, with the rates in nonsyndromic patients, nonsyndromic patients with Pierre Robin sequence, and syndromic individuals being 84%, 79%, and 58%. The investigators also found speech outcomes to be significantly worse in syndromic persons than in nonsyndromic ones. [8]
Relevant Anatomy
Z-plasty requires a proper skin thickness. A flap with too much subcutaneous tissue is difficult to position because of limited rotation. A thin flap contracts readily and is unattractive. Ideally, a plane developed between the subdermal plexus and the subcutaneous fatty tissue provides support but is not restrictive in the degree of rotation afforded.
Contraindications
When designing a local flap, consider any factor that may compromise expected results. Attempt to identify health risks that affect vascular supply to the skin (eg, atherosclerotic heart disease, diabetes, smoking, collagen vascular disease, prior irradiation, anticoagulation). A history of poor wound healing, hypertrophic scarring, or keloid formation is a relative contraindication to Z-plasty.
-
The original scar is A-B. The limbs of the Z-plasty form 2 triangles with 45° angles at apices C and D.
-
After transposition of C and D, the scar has reoriented 90° and lengthened. Note the increased distance between hooks, as well as the changed position of asterisks compared with the previous image.
-
The distance between the ends of the scar is increased as the tissue from the flaps is transposed.





