Background
Rocky Mountain spotted fever (RMSF) is a tick-borne disease caused by the organism Rickettsia rickettsii. Although RMSF can be lethal, it is curable. RMSF is the most common rickettsial infection. The organism is endemic in parts of North, Central, and South America, especially in the southeastern and south-central United States.
 In the United States, the American dog tick (Dermacentor variabilis) is the most commonly identified source of transmission. This tick is actually found mainly east of the Rocky Mountains. The Rocky Mountain wood tick (Dermacentor andersoni), found predominantly in the mountain states, can transmit RMSF and tularemia to humans. The brown dog tick (Rhipicephalus sanguineus) is a source of RMSF in the southwestern United States and along the US-Mexico border, but it is found throughout the country and the world. Courtesy of the Centers for Disease Control and Prevention (CDC).
In the United States, the American dog tick (Dermacentor variabilis) is the most commonly identified source of transmission. This tick is actually found mainly east of the Rocky Mountains. The Rocky Mountain wood tick (Dermacentor andersoni), found predominantly in the mountain states, can transmit RMSF and tularemia to humans. The brown dog tick (Rhipicephalus sanguineus) is a source of RMSF in the southwestern United States and along the US-Mexico border, but it is found throughout the country and the world. Courtesy of the Centers for Disease Control and Prevention (CDC).
Sophisticated microbiologic and serologic methods to distinguish infection by different members of the spotted-fever group reveal that RMSF may be more common in the tropics and subtropical regions of the Americas than previously thought.
RMSF has been described as a "wolf in sheep's clothing" and "the great imitator" of other disease processes. [1] Because of its diverse clinical features, RMSF is often confused with other infections. The hallmark of RMSF is a petechial rash beginning on the palms of the hands and soles of the feet.
 The patient's rash is a major diagnostic sign of Rocky Mountain spotted fever (RMSF). Courtesy of the Centers for Disease Control and Prevention (CDC).
The patient's rash is a major diagnostic sign of Rocky Mountain spotted fever (RMSF). Courtesy of the Centers for Disease Control and Prevention (CDC).
 An adult female Dermacentor variabilis (American dog tick). Courtesy of the Centers for Disease Control and Prevention (CDC) (https://www.cdc.gov/rmsf/index.html).
An adult female Dermacentor variabilis (American dog tick). Courtesy of the Centers for Disease Control and Prevention (CDC) (https://www.cdc.gov/rmsf/index.html).
See also 7 Bug Bites You Need to Know This Summer, a Critical Images slideshow, for helpful images and information on various bug bites.
The 2 principal tick vectors of RMSF in North America are Dermacentor variabilis (dog tick), in the eastern United States, and D andersoni, in the Rocky Mountain region and Canada. Other species also identified include Rhipicephalus sanguineus in Mexico and Central America and Amblyomma cajennense in Central and South America. A cooperi, A americanum, Ixodes pacificus, and Haemaphysalis leporispalustris are uncommon vectors for human infection.
Major Marshall H. Wood, a US Army physician in Boise, Idaho, first recognized R rickettsii infection and described RMSF in 1896. The first report in the medical literature of a case in the Snake River Valley of Idaho was published in 1899. In 1902, 7 people died of RMSF in Bitterroot Valley. Then, 111 cases of RMSF were studied on the west side of the Bitterroot River; 69% of these cases were fatal. Based on the history of tick exposure and the season, researchers concluded that the wood tick spreads RMSF.
Howard Ricketts, for whom the etiologic pathogen is named, identified R rickettsii, its vector, and the route of transmission of RMSF. In 1906, Ricketts demonstrated tick transmission of RMSF to guinea pigs, showed that the etiologic agent was present in blood from infected humans, and demonstrated that it could be removed via filtration. Ricketts reported "minute polar staining bacilli" in freshly laid eggs of infected ticks.
In 1916, Wolbach published 2 papers also describing the appearance of R rickettsii using the Giemsa stain. In 1919, he reported that R rickettsii is an intracellular pathogen, and he described the vasculitic lesion.
In the late 1940s, broad-spectrum antibiotics ̶ chloramphenicol and the tetracyclines ̶ were first shown to be effective in the treatment of RMSF.
Mortality rates as high as 30% were reported for RMSF in the preantibiotic era. Although its clinical manifestations and treatment of the disease are well known, RMSF still causes significant mortality and morbidity. The current mortality rate is 1.4%. A significant portion of this persistent mortality is likely due to delay in diagnosis and treatment.
Patient education
For patient education information, see Ticks.
Etiology and Pathophysiology
R rickettsii is a small (0.3 µm X 1 µm), gram-negative, obligate, intracellular coccobacillus. It possesses outer-membrane protein A (OmpA) and OmpB, 2 major immunodominant, surface-exposed proteins with species-specific conformational epitopes. OmpB is the most abundant outer-membrane protein that shares genetic sequences and limited antigens with typhus group rickettsiae.
Ticks become infected by feeding on the blood of infected animals, through fertilization, or by transovarial passage. Rickettsiae are transmitted from tick to human during feeding. The tick needs to be attached to a host for 6-10 hours for rickettsiae to be released from the salivary glands, although transmission may not occur for 24 hours. In addition, this organism can infect people who remove ticks from other people or animals via contact with tick tissues and fluids.
The organism spreads through the body via blood and the lymphatic system. The incubation phase of infection ranges from 3-12 days, depending on the volume of the inoculum.
Notable characteristics of R rickettsii include its marked tropism for endothelial cells that line blood vessels and its enhanced ability to invade throughout the body compared with other rickettsiae. The organisms attach via OmpA to the endothelial membrane, where they induce their own engulfment. Once they invade the cell and effectively escape destruction by professional phagocytes, they replicate via binary fission in the cytosol and spread from cell to cell, propelled by polar polymerization of the host cell's actin, without producing cell lysis.
The rickettsial diseases, especially Rocky Mountain spotted fever (RMSF), are model examples of vasculitis with localization in endothelial cells. The major pathophysiologic effect of endothelial cell injury is increased vascular permeability, which results in edema, hypovolemia, hypotension, and hypoalbuminemia. The organisms also routinely infect vascular smooth-muscle cells.
The distribution of rickettsiae within the blood vessels causes vascular injury and the subsequent development of a host mononuclear-cell tissue response. Consequences of vascular injury include interstitial pneumonia, interstitial myocarditis, and perivascular glial nodules of the central nervous system (CNS), with similar vascular lesions in the skin, gastrointestinal (GI) tract, pancreas, liver, skeletal muscles, and kidneys. Large amounts of rickettsiae in damaged cells support the concept of direct injury.
The inflammation and damage to the blood vessels and capillaries activate platelets, generate thrombin, and activate the fibrinolytic system as part of the body's homeostatic physiologic response to endothelial injury.
As R rickettsii proliferates in the endothelial lining, it also causes thrombi to form. In severe cases, extensive vasculitis can lead to small-vessel occlusion. Vascular necrosis and thrombosis are more common in RMSF than in typhus and may mimic collagen-vascular disease.
Epidemiology
Occurrence in the United States
Rocky Mountain spotted fever (RMSF) is the most common cause of fatal tick-borne disease in the United States. Anyone who is bitten by an infected dog tick and on whom the infected tick remains for several hours can develop RMSF. In spite of its name, RMSF is more common in the southeastern US tick belt than in the Rocky Mountain region. The disease is more common in rural and suburban locations; however, it does occur in urban areas such as New York City. [3, 4, 5, 6]
In the United States, the American dog tick (Dermacentor variabilis) is the most commonly identified source of transmission. The Rocky Mountain wood tick (Dermacentor andersoni), found predominantly in the mountain states, can transmit RMSF and tularemia to humans. The brown dog tick (Rhipicephalus sanguineus) has recently been identified as a source of RMSF in the southwestern United States and along the US-Mexico border, but it is found throughout the country and the world. Each dot represents one case. Cases are reported from the infected person’s county of residence, not necessarily the place where they were infected.
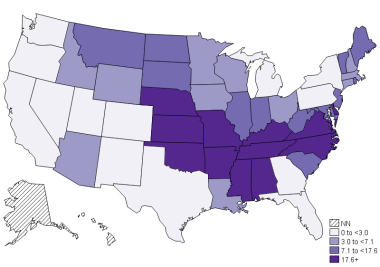 Annual incidence (per million persons) of Spotted Fever Rickettsiosis (SFR) in the United States, 2018. As of January 1, 2010, cases of Rocky Mountain Spotted Fever (RMSF) have been reported under a new category called Spotted Fever Rickettsiosis (SFR). Courtesy of the Centers for Disease Control and Prevention (CDC) (https://www.cdc.gov/rmsf/stats/index.html#anchor_1531851146113).
Annual incidence (per million persons) of Spotted Fever Rickettsiosis (SFR) in the United States, 2018. As of January 1, 2010, cases of Rocky Mountain Spotted Fever (RMSF) have been reported under a new category called Spotted Fever Rickettsiosis (SFR). Courtesy of the Centers for Disease Control and Prevention (CDC) (https://www.cdc.gov/rmsf/stats/index.html#anchor_1531851146113).
The regions with the highest incidences include the Southeast, the western South Central region (including Oklahoma and northern Texas), and selected areas of the Northeast (Cape Cod and Long Island). Most cases are reported from eastern and central states. Five states (North Carolina, Oklahoma, Arkansas, Tennessee, Missouri) account for over 60% of cases [6]
Cases have been reported in 48 states, with Vermont and Hawaii being the exceptions. Although cases can occur during any season, most cases reported illness in May through August (CDC/1). From 1989-1996, more than 4700 cases were reported in 46 states. Of these reported cases, 90% occurred between April and September. In the northern United States, infections commonly occur in the spring; in the South, cases may occur at any time of the year, including winter. This correlates during the season during which adult Dermacentor ticks are most active [6] .
A prospective study of RMSF infection in residents of a known endemic area in North Carolina suggested an annual incidence of 42 cases per 100,000 children aged 5-9 years. Asymptomatic infection may be common; in one study, 12% of children living in high-risk zones had positive serology test results, indicating past exposure to RMSF. [7]
In 2005, 1936 cases were reported—more than 4 times the 365 cases reported in 1998. The reasons for this increase are not known, but wide swings in the incidence of RMSF have occurred since 1920. Due to underdiagnosis, lack of testing, and lack of reporting, it is likely that the actual number of cases is much higher than surveillance data suggest.
RMSF has become increasingly more common in certain areas of Arizona. Between 2003 and 2018, approximately 430 cases were reported with an associated case-fatality rate of approximately 5%. [6]
International occurrence
Canada, Mexico, and Central and South America (particularly Panama, Columbia, Argentina, Costa Rica, Bolivia, and Brazil) have reported cases of RMSF. Serologic evidence of RMSF has been found in 6 Brazilian states, ranging from Rio Grande de Sol in the south to Bahia in the north. In Brazil, RMSF was unrecognized or unreported for decades in regions such as Espiritu Santo. In southern Brazil, the disease is more common from October to February, but, in the tropics, seasonal variation is less striking. [8]
There have been no documented cases of RMSF infection outside of the Americas. However, a wide range of related spotted fever group (SFG) rickettsioses has been described across Europe, Africa, Asia, and Oceania. The true incidence of spotted fever infections internationally is not known.
Race-related demographics
Whites have twice the incidence of African Americans; however, African Americans have a higher case-fatality rate. This may be due to the greater difficulty of appreciating a rash in highly pigmented individuals.
American Indians are at greater risk for RMSF than the general population. [9] From 2001-2005, the average annual incidence of RMSF reported among American Indians was 16.8 per 1,000,000 persons compared with 4.2 for whites, 2.6 for blacks, and 0.5 for Asian/Pacific Islanders. The incidence of RMSF in American Indians increased at a disproportionate rate during this period, although from 1990-2000, the rate was comparable to those for other races from 1990-2000. [10]
Sex- and age-related demographics
The male-to-female ratio for RMSF is 1.7:1. The mortality risk is also higher in males than in females.
The incidence of Rocky Mountain spotted fever is highest among adults aged 60-69 years (3.1 cases/million persons) and children aged 5-9 years (an estimated 3.3 cases/million persons).
Prognosis
Mortality rates in Rocky Mountain spotted fever (RMSF) vary according to the following criteria:
-
Delay in diagnosis
-
Delay in effective antibiotic treatment - In a 1995 study, antirickettsial therapy within the first 5 days of illness reduced the risk of mortality 5-fold compared with treatment initiation after the 5-day mark [11]
-
Age
-
Race
-
Gender - Mortality risk is higher in males
-
Severity of the disease
-
Presence of chronic alcohol abuse
-
Presence of glucose-6-phosphate-dehydrogenase deficiency
The mortality rate in untreated cases of RMSF is 20-25%. Mortality rates can be as low as 5% with proper antibiotic therapy and as high as 70% in untreated elderly individuals. Death in 5 days can be expected in fulminant cases. [4]
Complications
Complications may include the following [12, 13, 14] :
-
Disseminated intravascular coagulation
-
Noncardiogenic pulmonary edema
-
Acute tubular necrosis
-
Shock with myocarditis
-
Skin necrosis and gangrene - Particularly in fingers, toes, elbows, ears, and scrotum
-
Myocarditis - Usual cause of death
-
Seizures
-
Encephalopathy
-
Peripheral neuropathy
-
Bowel and bladder incontinence
-
Cerebellar and vestibular dysfunction
-
Hearing loss
-
Blindness - The frequency of long-term ocular sequelae is low; in most cases, good binocular visual acuity is preserved
-
Scarring
-
Hemophagocytic histiocytosis - Has been described in fatal cases of RMSF
Factors at presentation associated with development of acute renal failure (ARF) include increased bilirubin, advancing age, thrombocytopenia, and the presence of neurologic involvement. Age and decreased platelet count at presentation have been independently associated with the development of ARF by multivariate analysis. ARF development increases the odds ratio of dying by a factor of 17.
-
The patient's rash is a major diagnostic sign of Rocky Mountain spotted fever (RMSF). Courtesy of Springer Nature [Bal AK, Kairys SW. Kawasaki disease following Rocky Mountain spotted fever: a case report. Journal of Medical Case Reports. 2009;3:7320. Available at: http://www.jmedicalcasereports.com/content/3/1/7320. Accessed July 25, 2013.]
-
The patient's rash is a major diagnostic sign of Rocky Mountain spotted fever (RMSF). Courtesy of the Centers for Disease Control and Prevention (CDC).
-
In the United States, the American dog tick (Dermacentor variabilis) is the most commonly identified source of transmission. This tick is actually found mainly east of the Rocky Mountains. The Rocky Mountain wood tick (Dermacentor andersoni), found predominantly in the mountain states, can transmit RMSF and tularemia to humans. The brown dog tick (Rhipicephalus sanguineus) is a source of RMSF in the southwestern United States and along the US-Mexico border, but it is found throughout the country and the world. Courtesy of the Centers for Disease Control and Prevention (CDC).
-
An adult female Dermacentor variabilis (American dog tick). Courtesy of the Centers for Disease Control and Prevention (CDC) (https://www.cdc.gov/rmsf/index.html).
-
Annual incidence (per million persons) of Spotted Fever Rickettsiosis (SFR) in the United States, 2018. As of January 1, 2010, cases of Rocky Mountain Spotted Fever (RMSF) have been reported under a new category called Spotted Fever Rickettsiosis (SFR). Courtesy of the Centers for Disease Control and Prevention (CDC) (https://www.cdc.gov/rmsf/stats/index.html#anchor_1531851146113).





