Overview
Rabies, a viral disease of the central nervous system (CNS), is widespread throughout the world. (See the image below.)
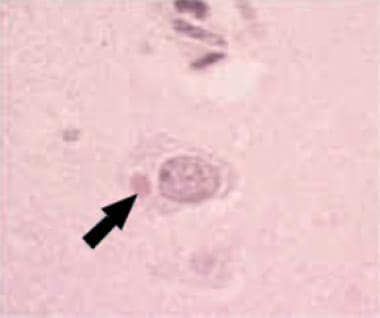 Hematoxylin and eosin stain of Negri body in a rabies-infected neuron. Courtesy of the US Centers for Disease Control and Prevention.
Hematoxylin and eosin stain of Negri body in a rabies-infected neuron. Courtesy of the US Centers for Disease Control and Prevention.
Treatment of rabies should be based on history and exposure. One should not withhold treatment while waiting for diagnostic tests.
Go Rabies for complete information on this topic.
Emergency Department Care
Treatment discussed here focuses on animal exposures where rabies transmission is a possibility. This is the primary concern of the emergency physician. Treatment of human rabies is supportive and often involves therapy for other possible etiologies before specific diagnosis is made, usually postmortem or well into an intensive care unit (ICU) hospitalization.
Eliciting a history of recent animal or bite exposures is of utmost importance, as many patients described in the literature were initially sent home by the emergency department.
Postexposure prophylaxis (PEP) consists of wound cleaning, vaccination, and administration of rabies immunoglobulin.
Wound Cleaning
Immediate therapy, provided prior to the administration of vaccine and immunoglobulin, consists of the thorough cleaning of all bite and scratch wounds with soap and water, 2% benzalkonium chloride, and/or a virucidal agent (ie, povidone-iodine solution). Wound cleaning alone has been shown to reduce the likelihood of rabies transmission in animal studies. Provide wound care as needed; tetanus prophylaxis usually is indicated, as are measures to prevent bacterial infection. When appropriate, wound closure should be avoided. [1]
Vaccines
The 2 rabies vaccines currently available in the United States are the human diploid cell vaccine (HDCV, Imovax) and the purified chick embryo cell vaccine (PCECV, RabAvert). Both are made for intramuscular administration and are equal in efficacy and safety. The vaccine takes 7-10 days to induce an active immune response, with immunity lasting approximately 2 years.
Once a vaccination series is initiated, it usually is completed with the same vaccine product, although no trials have been done to study the effects (beneficial or adverse) of beginning with one and ending with another. [1]
Slight erythema may be expected with both vaccines, but any further skin changes should be reported to the health department to determine actual necessity of vaccine.
No postexposure vaccine failures in the United States have been reported since HDCV was licensed in 1980. Of 13 cases of postexposure treatment failure that occurred outside the United States, all were from not cleaning wounds, not giving rabies vaccine, or giving rabies vaccine into the gluteal region rather than the deltoid region.
Rabies Immunoglobulins
Passive immunization with human rabies immunoglobulin (HRIG, HyperRab S/D, KedRab, Imogam Rabies-HT) provides immediate protection.
The immunoglobulin elicits neutralizing antibodies and has a half-life of 21 days.
Products are from hyperimmunized human donor plasma and could potentially contain infectious agents, although this risk is small secondary to initial screening of donors. Currently, no documented transmission of adventitious agents exists. [1]
Neural tissue rabies vaccines should no longer be used, although they may still be used in some developing countries.
In countries that cannot afford the 5-dose regimen, the World Health Organization (WHO) states that 2 regimens are available that fulfill their requirements. These have been used in developing countries as replacements for the more expensive injections. These injections should be administered in consultation with the Centers for Disease Control and Prevention (CDC).
Postexposure Prophylaxis in Previously Unvaccinated Immunocompetent Persons
Human rabies immunoglobulin
Administer 1 dose (20 IU/kg) to produce virus-neutralizing antibodies. Administer on Day 0 at the same time as the vaccine. If not immediately available, the HRIG should be administered as soon as it becomes available up until and including day 7 of treatment. Concentrate as much of the dose as possible in and around the wound (if wound location allows). The remaining HRIG should be administered intramuscularly at a site distant from the vaccine administration. [2]
Case reports have documented safe administration of HRIG and HDCV during pregnancy.
Vaccine
Four doses (1 mL each) of either HDCV or PCECV vaccine should be administered on Days 0, 3, 7, and 14. The first dose should be administered as soon as possible after exposure. It should be given intramuscularly into the deltoid muscle of adults. In children, it should be administered into either the deltoid muscle or the anterolateral aspect of the thigh. Do not use the gluteal region, because this could result in a decreased immunologic response. It is important to give all 4 doses. [2]
Postexposure Prophylaxis in Immunocompromised Persons
Immunocompromised persons should receive HRIG and the vaccine as described above but should, in addition, receive a fifth dose, on Day 28. Any immunosuppressive agents should be stopped during rabies PEP unless necessary and essential for management of another condition.
Additionally, serum should be tested to document seroconversion 1-2 weeks after completing PEP. The rapid fluorescent focus inhibition test (RFFIT) should be used to determine that an appropriate antibody response has developed. If the patient does not seroconvert, the patient should continue management with both the physician and public health officials. [2]
Postexposure Prophylaxis in Previously Vaccinated Persons
Previously vaccinated persons include those who have received the 3-dose preexposure series of HDCV, rabies adsorbed virus (RVA), or PCECV; a full PEP; or a previous vaccination with any rabies vaccine with a documented history of seroconversion.
HRIG should not be administered.
For the vaccine, administer 2 doses (1 mL each) into the deltoid muscle on Day 0 and Day 3.
-
Hematoxylin and eosin stain of Negri body in a rabies-infected neuron. Courtesy of the US Centers for Disease Control and Prevention.




