Practice Essentials
Amphetamines are a class of compounds that are abused in many regions of the world, including the United States, Australasia, and Europe. Synthetic amphetamine compounds commonly are produced in clandestine laboratories and vary in purity and potency. Other potentials for amphetamine abuse include prescription medications often used for attention deficit disorder and various over-the-counter diet pills.
Clinical effects of amphetamine abuse are significant and commonly observed in emergency departments (EDs). [1] Hendrickson et al found that about 2.4% of visits at their institution were related to methamphetamine use and generated annual estimated hospital costs of $6.9 million. [2] Patients may present with a range of psychiatric and medical problems, including agitation, psychosis, seizures, and potentially life-threatening cardiac dysrhythmias; see Presentation, Workup, and Treatment.
See also Methamphetamine Toxicity and MDMA Toxicity.
Pathophysiology
Amphetamines are a group of structurally related compounds that produce central nervous system (CNS) and peripheral nervous system (PNS) stimulation. The phenylethylamine structure of amphetamines (see the image below) is similar to catecholaminergic, dopaminergic, and serotonergic agonists (biogenic amines), which may explain their actions.
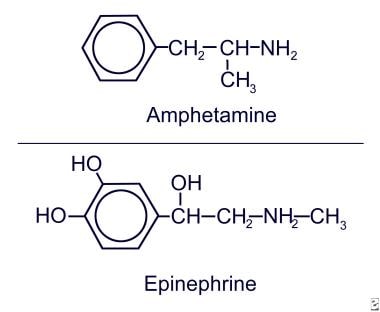 Amphetamine and epinephrine.
Amphetamine and epinephrine.
The degree to which an amphetamine can stimulate the receptors of these biogenic amines depends on the chemical substituents on the amphetamine molecule; thus, the clinical presentation depends on the type of amphetamine used. For example, methamphetamine lacks much of the peripheral stimulant properties of amphetamine while still offering euphoric and hallucinogenic properties. These actions are similar to those of cocaine; however, while effects of cocaine last for 10-20 minutes, duration of amphetamine action is much longer—as long as 10-12 hours.
The routes of amphetamine administration may be oral (ingestion), inhalation (smoke), or injection (intravenous). Oral use is associated with an approximate 1-hour lag time before onset of symptoms, whereas inhaled and intravenous methods yield effects within a few minutes. Peak plasma concentrations occur in 5 minutes with intravenous use, 30 minutes with nasal or intramuscular use, and 2-3 hours postingestion.
Use appears to vary with gender and race. Research has found correlations between personality traits (risk taking and reward sensitivity) and responses to amphetamine use. [3]
Central nervous system
Amphetamine compounds cause a general efflux of biogenic amines from neuronal synaptic terminals (indirect sympathomimetics). They inhibit specific transporters responsible for reuptake of biogenic amines from the synaptic nerve ending and presynaptic vesicles. Amphetamines also inhibit monoamine oxidase, which degrades biogenic amine neurotransmitters intracellularly. The net effect is an increase of neurotransmitter release into the synapse. Physiologic adaptation occurs through receptor or coupling down-regulation; this tolerance and an accompanying psychological tolerance [4] can lead to escalating use of the drug and increased toxicity. [5] Long-term use can lead to a depletion of biogenic amine stores and a paradoxical reverse effect of the drug—a washout.
Elevated catecholamine levels usually lead to a state of increased arousal and decreased fatigue. Increased dopamine levels at synapses in the CNS may be responsible for movement disorders, [6] schizophrenia, and euphoria. Serotonergic signals may play a role in the hallucinogenic and anorexic aspects of these drugs.
Other serotonergic and dopaminergic effects may include resetting the thermal regulatory circuits upward in the hypothalamus and causing hyperthermia. [7] The hyperthermia produced by amphetamines is similar to that of the serotonin syndrome.
Laboratory studies reveal that amphetamines interfere with the normal control of the neurohumoral (hypothalamopituitary) axis, affecting secretion of such factors as adrenocorticotropic hormone (ACTH). Amphetamines may alter other neural functions such as complex behavioral and learning patternings; this may be important for understanding effects of amphetamine use on the fetus during pregnancy.
Animal studies indicate that amphetamines interact with N-methyl-D-aspartate (NMDA) receptors on serotonergic neurons, leading to neuronal destruction. This interaction may contribute to seizure activity.
In vitro, amphetamines have been found to stimulate regulatory molecules, such as the oncogenes c-fos and ras and cyclic adenosine monophosphate (cAMP) response element binding (CREB) protein. Amphetamines have been found to act on ras-mediated striatal motor control. [8] These proteins are responsible for signaling long-term changes at the transcriptional level.
Cardiovascular
Catecholaminergic (sympathomimetic) effects of amphetamines include inotropic and chronotropic effects on the heart, which can lead to tachycardia and other dysrhythmias. The vasoconstrictive properties of the drugs can lead to hypertension and/or coronary vasospasm. [9]
Serotonergic action of amphetamines on peripheral vasculature can lead to vasoconstriction, which is especially problematic in placental vessels. Animal studies have shown that serotonergic actions of amphetamines effect changes in plasma levels of oxytocin, somatostatin, gastrin, and cholecystokinin. [10]
Long-term use of the drugs can lead to myonecrosis and dilated cardiomyopathy. [11, 12] Amphetamine use is also associated with myocardial infarction [13]
Etiology
Marked tolerance develops after amphetamine use and leads to rapid escalation of drug doses. Increasing the dose produces increasing toxicity and complications from acute and chronic amphetamine use.
Epidemiology
Frequency
United States
Accurate estimation of illicit amphetamine use is difficult. An estimated 13 million Americans use these compounds without medical supervision. Random toxicologic screens performed in the ED indicate amphetamine presence in about 2% of patients. The 2022 Annual Report of the American Association of Poison Control Centers' National Poison Data System noted 9931 single exposures with 1640 moderate outcomes, 140 major outcomes, and one death. [14]
According to National Institute on Drug Abuse estimates for 2020, 6% of 8th graders, 5.4% of 10th graders, and 5.3% of 12th graders had used amphetamines during the past year. [15] Self-reporting among college students indicates an approximate 4% prevalence. An age-matched survey of fourth-year medical students revealed that about 1.2% use amphetamines. It is unclear how many of these uses are of amphetamine-containing prescriptions for attention deficit disorder (ADD) or attention deficit hyperactivity disorder (ADHD).
International
According to the United Nations Office on Drugs and Crime (UNODC) World Drug Report, global seizures of amphetamine reached a record high in 2019, with 49% of seizures in the Near and Middle East/South and West Asia. Western and Central Europe accounted for 26% of seizures. [16] The UNODC estimates that worldwide, there were 36 million users of amphetamines and prescription stimulants in 2021. [17]
Race- and sex-related demographics
Amphetamine use characteristically occurs among single White men aged 20-35 years who are typically unemployed. [18] Data from rural populations reveal that Whites use amphetamines significantly more than Blacks. [19] However, among 12th grade students, the annual prevalence of amphetamine use is highest in Blacks (3%), followed by Hispanics (2%). White 12th grade students had the lowest prevalence, at 1%. [15]
According to the National Institute on Drug Abuse, the prevalence of amphetamine use is higher among females than among males in 8th grade, but nearly equal by 12th grade. This is explained partially by their higher use in 8th-grade girls to aid in weight loss. [15]
One study suggests that the action of estrogen within the CNS might explain why fewer women than men use amphetamines. Women in their late follicular phase (when estrogen levels are high and progesterone levels are low) were more likely to report "unpleasant stimulation" when exposed to amphetamine. This effect was not observed in the early follicular phase, when both hormone levels are low. [20]
Prognosis
Patients without signs or symptoms of end-organ failure or infections may do well with sedation and reassurance. No established modalities exist for treatment of amphetamine addiction.
Hyperthermia accompanies and complicates significant amphetamine intoxication. Liver damage apparently is linked to elevated body temperature and consumption of reduced glutathione in metabolism of amphetamines. Because amphetamines often are synthesized in poorly controlled settings, individuals with amphetamine intoxication may experience concomitant toxic exposures. Lead, other metals, organic solvents, and precursor molecules all have been found in amphetamine samples and blood of individuals with amphetamine toxicity.
Acute overdose of amphetamines can result in the following:
-
Seizures
-
Hypertension
-
Tachycardia
-
Myocardial infarction [21]
-
Hyperthermia
-
Psychosis [22]
-
Hallucinosis
-
Stroke
-
Death
Habitual amphetamine use produces toxic psychosis resembling paranoid schizophrenia. Hallucinations, delusions, and bizarre violent behavior are common. In a few patients, amphetamine use produces long-term paranoid schizophrenia; whether this results from unmasking underlying disease is unclear. Severe psychological depression and prolonged sleep follow chronic use and binges.
Amphetamine abuse during pregnancy has been linked with adverse outcomes in offspring. [23, 24] However, use of prescribed medication for ADHD during pregnancy appears to be safe. [25]
Patient Education
Educate patients on the toxic effects of amphetamines and that amphetamines are not a safe alternative to cocaine use. For patient education information, see the First Aid and Injuries Center and Mental Health Center, as well as Drug Dependence & Abuse, Poisoning, Club Drugs, Activated Charcoal, and Substance Abuse.
-
Amphetamine and epinephrine.








