Practice Essentials
Fractures of the hip are relatively common in adults and often lead to devastating consequences. Disability frequently results from persistent pain and limited physical mobility. Most hip fractures occur in elderly individuals as a result of minimal trauma, such as a fall from standing height. In young, healthy patients, these fractures usually result from high-velocity injuries, such as motor vehicle collisions or falls from significant heights. Despite comparable fracture locations, the differences in low- and high-velocity injuries in older versus younger patients outweigh their similarities. High-velocity injuries are more difficult to treat and are associated with more complications than minor trauma injuries.
Hip fracture occurs in approximately 341,000 persons in the United States each year, [1] with an estimated mortality of 14-36%. [2, 3, 4] The rate of hip fracture increases with age, doubling every 5-6 years after age 60 years. [1] Hip fractures are associated with substantial morbidity and mortality; approximately 15-20% of patients die within 1 year of fracture. Interestingly, morbidity and mortality for those older than 90 years sustaining a hip fracture have not been found to be statistically higher than others in the same age group without such an injury. Worldwide, the rate of hip fracture is approximately 150 per 100,000 persons in North America and Europe. Early diagnosis is important because mortality doubles with delay of surgery of more than 2 days. [2, 3, 4]
(See the image below.)
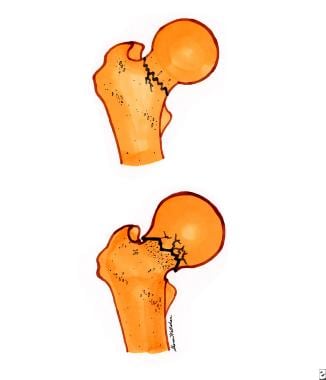 Femoral neck fractures. Top diagram is a nondisplaced, or incomplete, femoral neck fracture. Bottom diagram is an impacted femoral neck fracture.
Femoral neck fractures. Top diagram is a nondisplaced, or incomplete, femoral neck fracture. Bottom diagram is an impacted femoral neck fracture.
Signs and symptoms
In elderly patients, hip fracture most often results from a simple fall. The patient typically complains of pain and inability to move the hip.
With stress fractures in young athletes and nondisplaced fractures, the patient may complain of pain in the hip or knee and may be ambulatory.
On physical examination, the anatomic position of the extremity provides useful clues to the type of injury, as follows:
-
Femoral head fracture: Posterior dislocation is most common (eg, a dashboard injury), in which case the extremity appears adducted and internally rotated; with anterior dislocation, the extremity is abducted and externally rotated.
-
Femoral neck fracture: With partial or completely displaced fractures (types 3 and 4, respectively), the patient has severe pain and lies with the extremity slightly shortened, abducted, and externally rotated; with a stress fracture or severe impaction fractures (types 1 and 2, respectively), the only physical findings may be minor pain with little or no limitation in range of motion.
-
Trochanteric fracture: With a greater trochanteric fracture, the patient presents with pain, especially with abduction and extension; no deformity may be apparent, but pressure through greater trochanters will result in pain; with a lesser trochanteric fracture, pain occurs during flexion and internal rotation.
-
Intertrochanteric fracture: The extremity appears shortened and significantly externally rotated, in contrast to the minimal deformities associated with femoral neck fractures; pain, hip edema and ecchymosis, and pain with any movement may also be noted..
-
Subtrochanteric fracture: The proximal femur usually is held in flexion and external rotation.
Diagnosis
On plain radiographs, anteroposterior (AP) and lateral views demonstrate most hip fractures. For patients in whom femoral neck fracture is strongly suspected but standard radiographic findings are negative, an AP view with internal rotation provides a better view of the femoral neck. [5, 6, 7]
If standard radiographic findings are negative and hip fracture still is strongly suspected, MRI and bone scan have high sensitivity in identifying occult injuries; MRI is 100% sensitive in patients with equivocal radiographic findings. When MRI is contraindicated, CT is an appropriate alternative. [5]
Classifications
The Pauwel classification divides fractures into 3 groups based on the angle of the fracture from the horizontal plane, as follows [6, 8, 9, 10] :
-
Type 1: < 30 degree
-
Type 2: 31-50 degrees
-
Type 3: >50 degrees
The Garden classification describes 4 fracture patterns for intracapsular fractures and defines them based on the completeness and displacement of the fracture, as follows [6, 8, 9, 10] :
-
Type 1: incomplete fracture and no displacement
-
Type 2: complete fracture and no displacement
-
Type 3: complete fracture and partial displacement
-
Type 4: complete fracture and complete displacement
The Evans classification of intertrochanteric fractures is based on the location and direction of the fracture as well as the stability of the fracture. [11]
Extracapsular fractures are typically described using the AO classification, as follows [6, 8, 9, 10] :
-
A1: 2-part, stable fracture
-
A2: comminuted, unstable fracture
-
A3: reverse or transverse, unstable fracture
Management
Femoral head fractures
Treatment of type 1 femoral head fractures is as follows:
-
Obtain orthopedic consultation in the ED.
-
Reduce dislocated femoral head and fracture fragment as soon as possible to avoid avascular necrosis.
-
Small fracture fragments may need to be removed.
-
If a single attempt at closed reduction fails, open reduction and internal fixation (ORIF) is the next treatment of choice.
For type 2 femoral head fractures, early orthopedic consultation for admission and arthroplasty is recommended.
Femoral neck fractures
-
Type 1: Some practitioners handle these fractures nonoperatively with initial immobilization in selected patients, while others prefer operative treatment in all patients.
-
Types 2, 3, and 4: Management usually includes ORIF or arthroplasty; however, some impacted fractures can be treated conservatively; early orthopedic consultation is recommended.
Trochanteric fractures
-
Type 1: Management is most often conservative, and orthopedic consultation is recommended
-
Type 2: These fractures usually are treated with ORIF, except in older or debilitated patients in whom conservative treatment is appropriate
Intertrochanteric fractures
-
Apply traction or a traction splint.
-
Note the potential for significant blood loss; IV fluid resuscitation is generally recommended.
-
Stable and unstable fractures usually are treated with ORIF unless the patient is not an operative candidate for other reasons.
-
Early orthopedic consultation is recommended.
Subtrochanteric fractures
-
Significant hemorrhage is common, and IV fluid resuscitation is frequently necessary.
-
ED application of traction or traction splint is necessary.
-
Properly evaluate the entire patient to rule out associated severe injuries.
-
Consult orthopedic surgeon for admission and ORIF for most patients.
Localized nerve blocks, specifically fascia iliaca nerve block (FICB) and femoral nerve blocks (FNBs) , have been shown to be safe and effective in managing acute hip fracture pain in geriatric patients, leading to decreased opioid use. [12, 13, 14, 15]
Risk factors
Egan et al identified several risk factors associated with the risk of a hip fracture patient sustaining a second fall. [16] Increasing age, cognitive impairment, decreasing bone mass, decreasing depth perception, decreased mobility, dizziness, and a poor/fair self-perceived state of health were all linked to increasing likelihood of sustaining a second fall and thus a possible second hip fracture.
Several studies have identified additional risk factors for hip fracture. Sennerby et al identified generalized cardiovascular disease as a significant risk factor for hip fracture, [17] while Carbone et al determined that heart failure is a specific risk for hip fracture [18] . Specific characteristics in men were evaluated to determine the relationship to hip fracture; smoking, tall stature, stroke, and dementia were found to increase the risk of hip fracture, while non–work-related physical activity and high BMI were found to be protective. [19] Kettunen at al studied previously elite male athletes and found that these individuals sustained hip fractures at significantly older ages than their less active counterparts. [20]
Two medication classes have also been implicated in hip fractures. Nursing home patients on antipsychotic medications and HIV-positive patients on protease inhibitor therapy were more likely to sustain fractures than those on other agents. [21, 22]
For more information, see Medscape's Fracture Resource Center.
Skeletal Anatomy
The hip joint is a large multiaxial ball-and-socket synovial joint, enclosed by a thick articular capsule. The hip joint is designed for stability and a wide range of movement. Next to the shoulder, it is the most moveable of all joints. During standing, the entire weight of the upper body is transmitted to the heads and necks of the femurs. The round head of the femur articulates with the cuplike acetabulum. The depth of the acetabulum is increased by the reinforcing fibrocartilaginous labrum, which "grasps" the femoral head, covering more than half of it. Articular cartilage covers the entire head of the femur, except for the pit (fovea) for the ligament of the femoral head.
The strong, loose fibrous capsule permits free movement of the hip joint, attaching proximally to the acetabulum and transverse acetabular ligament. The fibrous capsule attaches distally to the neck of the femur only anteriorly at the intertrochanteric line and root of the greater trochanter. Posteriorly, the fibrous capsule crosses to the neck proximal to the intertrochanteric crest without attaching to it. The fibrous capsule thickens to form 3 ligaments of the hip joint: the Y-shaped iliofemoral ligament (of Bigelow), the pubofemoral ligament, and the ischiofemoral ligament.
The hip joint is further supported by the femur and the muscles that cross the joint; this bone and these muscles are the largest and most powerful in the human body. (The anatomy of the femur is shown below.)
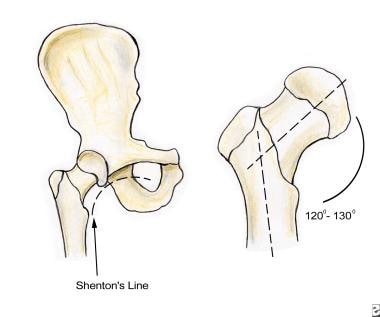
The length, angle, and narrow circumference of the femoral neck permit substantial range of motion at the hip but also subject the femoral neck to incredible shearing forces. A fracture results when these forces exceed the strength of the bone. The intertrochanteric line is an oblique line that connects the greater and lesser trochanters, dividing the femoral neck from the shaft. Hip fractures involve fracture of any aspect of the proximal femur, from the head to the first 4-5 cm of the subtrochanteric area.
Vascular Supply
The vascular supply to the proximal femur is tenuous and provided largely by 2 sources. Branches of the medial and lateral circumflex femoral arteries, usually branches of the deep femoral artery, ascend on the posterior aspect of the femoral neck in the retinacula (reflections of the capsule along the neck of the femur toward the head). The branches of the medial and lateral circumflex arteries perforate the bone just distal to the head of the femur, where they anastomose with branches from the foveal artery and with medullary branches located within the shaft of the femur.
The ligament of the head of the femur usually contains the artery of the ligament of the head of the femur (foveal artery), a branch of the obturator artery. The foveal artery enters the head of the femur only when the center of the ossification has extended to the pit (fovea) for the ligament of the head, around age 11-13 years. This anastomosis persists even in advanced age but is never established in 20% of the population.
Femoral neck fractures often disrupt the blood supply to the head of the femur. The medial circumflex artery supplies most of the blood to the head and neck of the femur and is often torn in femoral neck fractures. In some cases, the blood supplied by the foveal artery may be the only blood received by the proximal fragment of the femoral head. If the blood vessels are ruptured, the fragment of bone may receive no blood and undergo avascular necrosis (AVN).
Classifying Fractures
Hip fractures can be classified based on their relation to the hip capsule (intracapsular and extracapsular), geographic location (head, neck, trochanteric, intertrochanteric, and subtrochanteric), and degree of displacement. Higher-grade displacement implies worse prognosis. Fractures of the femoral head and neck are intracapsular, whereas those of the trochanteric, intertrochanteric, and subtrochanteric regions are extracapsular. The treatment, as well as the prognosis for successful union and restoration of normal function, varies considerably with fracture type.
Intracapsular hip fractures, like all other intracapsular fractures, frequently have complicated healing. The thick capsule that surrounds these fractures separates them from adjacent soft tissue and capillaries, leading to impaired callous formation. Thus, nonunion and AVN are added complications of these fractures.
Femoral head fractures
Isolated femoral head fractures are rare and are usually associated with hip dislocations. Superior femoral head fractures are normally associated with anterior dislocations, while inferior femoral head fractures are associated with posterior dislocations. They are usually best appreciated on postreduction radiographs for hip dislocations. Fractures of the femoral head are more common in younger patients as a result of major trauma, which is more likely to cause femoral neck fractures in older patients.
A type 1 fracture is a single fragment fracture, and type 2 is a comminuted fracture (see image below).
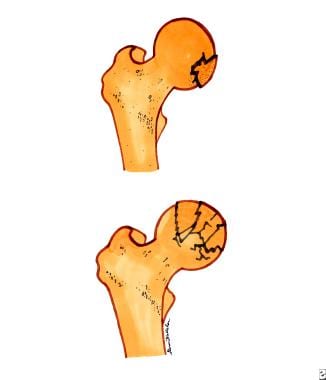 Femoral head fractures. Top diagram is a single-fragment femoral head fracture. Bottom diagram is a comminuted femoral head fracture.
Femoral head fractures. Top diagram is a single-fragment femoral head fracture. Bottom diagram is a comminuted femoral head fracture.
Femoral neck fractures
Femoral neck fracutures are rare in younger patients and more commonly seen in older adults, most often secondary to osteoporosis or osteomalacia. These fractures usually result from minor trauma, with falls accounting for 90%, or torsion. From proximal to distal, femoral neck fractures can be further delineated as subcapital, transcervical, and basicervical, all of which are intracapsular and are associated with potential disruption of the vascular supply. The incidence of avascular necrosis (AVN) is up to 15% in nondisplaced fractures and increases to nearly 90% with untreated, completely displaced fractures.
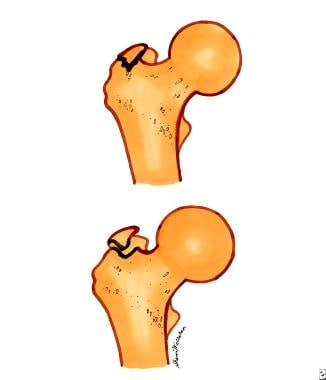
Type 1 is a stress fracture or incomplete fracture, and type 2 is an mpacted fracture (see image below).
Femoral neck fractures. Top diagram is a nondisplaced, or incomplete, femoral neck fracture. Bottom diagram is an impacted femoral neck fracture.
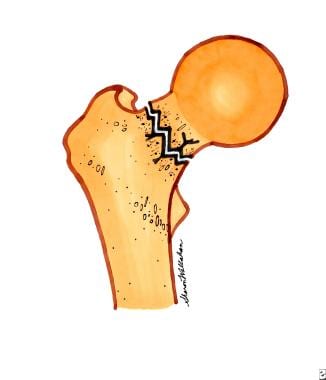
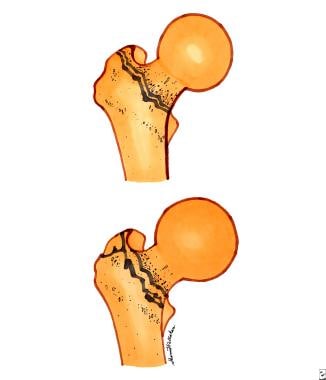
Type 3 is a partially displaced fracture (see image below).
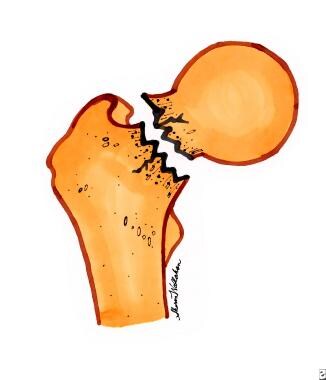
Type 4 is a completely displaced or comminuted fracture (see image below).
Trochanteric fractures
Greater trochanteric fractures usually result from avulsion injuries at the insertion of the gluteus medius. Lesser trochanteric fractures may be caused by avulsion injuries of the iliopsoas secondary to forceful contraction. These are most common in children and young athletes (eg, dancers, gymnasts).
Type 1 is a nondisplaced fracture, and type 2 is a displaced fractures, with >1 mm displacement for fractures of the greater trochanter and >2 mm displacement for fractures of the lesser trochanter (see image below).
 Trochanteric fractures. Top diagram is a nondisplaced trochanteric fracture. Bottom diagram is a displaced trochanteric fracture.
Trochanteric fractures. Top diagram is a nondisplaced trochanteric fracture. Bottom diagram is a displaced trochanteric fracture.
Intertrochanteric fractures
Intertrochanteric fractures are extracapsular fractures that occur in a line between the greater and lesser trochanters, generally in elderly patients and in women secondary to osteoporosis. Type 1 is a single fracture line without displacement and is stable; type 2 has multiple fracture lines (comminution) with displacement and is unstable (see image below).
 Intertrochanteric fractures. Top diagram is a single fracture line intertrochanteric fracture. Bottom diagram is a displaced, or multiple fracture line, intertrochanteric fracture.
Intertrochanteric fractures. Top diagram is a single fracture line intertrochanteric fracture. Bottom diagram is a displaced, or multiple fracture line, intertrochanteric fracture.
Subtrochanteric fractures
Subtrochanteric fractures have a bimodal age distribution and are seen most often in those aged 20-40 years, in association with high-energy trauma, and in patients older than 60 years secondary to falls on osteoporotic bones. It may be stable (bony contact of medial and posterior femoral cortices) or unstable.
Frequency
In the United States, hip fracture occurs in approximately 341,000 persons each year. [1] The rate of hip fracture increases with age, doubling every 5-6 years after age 60 years. [1] The fracture rate does decrease slightly after age 85 years. [1] Nearly half of all hip fractures occur in adults older than 80 years. Hip fracture at a young age is rare and is usually the result of a high-velocity injury or, rarely, secondary to bone pathology.
The US frequency of hip fracture, when age and sex are adjusted, ranks the highest in the world. Western Europe and New Zealand also have reported high rates, with the lowest rates occurring in the South African Bantu people and in East Asian countries, where the incidence of osteoporosis is low.
Mortality/Morbidity
Reported overall mortality rate of hip fractures is 15-20%, yet in older persons this can increase to 36% over the year following hip fracture. Rate of mortality is greatest in the first few months following injury but remains high for up to 1 year. It then returns to the same rate for age- and sex-matched people without hip fracture. Surgical delay independently affects mortality. Patients for whom surgery is delayed for 2 days or more have a 17% higher mortality at 1 month. A subsequent study showed increased mortality but decreased readmission rate in those in whom repair was done more than 4 days after injury. [23] Also, general anesthesia was associated with higher morbidity than was spinal/epidural anesthesia. [23]
Morbidity associated with hip fracture is staggering, especially in older persons. Morbidity from immobilization includes development of deep vein thrombosis, pulmonary embolism, pneumonia, and muscular deconditioning. Morbidity from surgical procedures includes complications of anesthesia, postoperative infection, loss of fixation, and malunion or nonunion, as well as the complications associated with immobilization. As many as 20% of patients return to the emergency department in the year following a hip fracture with concerns relating to morbidity associated with the initial fracture. [24]
Surgical delay of more than 48 hours has been shown to increase morbidity and mortality. [25]
Hip fracture resulting from major trauma often is associated with other bone and soft-tissue injuries, intra-abdominal and intrapelvic injuries, major blood loss, head and neck injuries, and other extremity injuries. Morbidity associated with an inability to return to a prefracture level of mobility results in a loss of independence, reduction in quality of life, and depression, particularly in older persons.
The incidence of hip fracture is 2-3 times greater in whites than in nonwhites, primarily because of the increased rate of osteoporosis in whites. This difference is not unique to females; African American and Asian men have been found to have significantly higher bone densities than their Caucasian and Latino counterparts. [26]
Rate of hip fracture is 2-3 times greater in women than in men. At least 75% of all hip fractures occur in women. The lifetime risk of hip fracture in white women and men is 15% and 5%, respectively. Femoral neck fractures are more common in women than in men by about 4:1, while intertrochanteric fractures are more common in women than in men by about 5:1.
The rate of recurrent injury in elderly patients with isolated hip fracture can be very high. Cabalatungan et al found that the rate of trauma related recidivism in patients 65 years or older with hip fracture was 8.9% (87 of 974). The majority of patients with hip fracture were women (first injury, 74.7%; second injury, 66.5%). Low-level fall was the most common cause of injury (95.4%). [27]
In a Swedish study by Ioannidis et al, hip fracture patients with dementia had a higher risk of death in the first 30 days after surgery. The adjusted risk of all-cause 30-day postoperative mortality was 67% higher in patients with dementia than in patients without dementia. Patients with dementia had a sevenfold increased risk of cerebrovascular-associated mortality. [28]
In a German prospective study by Knauf et al, 5-year survival of patients 60 years or older with hip fracture was 38% (152/395). Risk factors included older age, lower Mini-Mental State Examination, and the presence of delirium during hospitalization. [29]
Complications associated with hip fracture include the following [6, 30] :
-
Delirium: 13.5-33%
-
Pulmonary embolism: 1.4%-7.5%
-
Deep venous thrombosis: 27%
-
Pneumonia: 7%
-
Myocardial infarction or heart failure: 35-42%
-
Urinary retention or infection: 12-61%
-
Acute kidney injury: 11%
-
Anemia: 24-44%
-
Skin pressure damage: 7-9%
Prognosis
Hip fracture outcomes vary considerably depending upon the patient's age, comorbidities, fracture type, and numerous other factors.
In general, young patients almost always regain the ability to ambulate, yet depending on fracture type, they may not return to their previous level of activity.
Many older patients do not regain the ability to ambulate or are able to do so only with assistance. This profoundly affects their ability to live independently.
Almost 20% of patients never regain the ability to ambulate, and a similar percentage are unable to ambulate outside their homes.
Only 50-65% regain their premorbid ambulatory status.
The rate of recurrent injury in elderly patients with isolated hip fracture can be very high. Cabalatungan et al found that the rate of trauma related recidivism in patients 65 years or older with hip fracture was 8.9% (87 of 974). The majority of patients with hip fracture were women (first injury, 74.7%; second injury, 66.5%). Low-level fall was the most common cause of injury (95.4%). [27]
Patient Education
Prevention of hip fracture is vastly superior to current treatment modalities. Gear patient education toward identification of avoidable risk factors in the patient's life.
In young persons, stress avoidance of tobacco and alcohol abuse and safe, responsible use of motorized vehicles.
Counsel older persons on ways to make their home environment safe from falls. Encourage them to consult with their primary physician regarding medications or supplements for the prevention and treatment of osteoporosis.
For patient education resources, see Hip Pain and Bone Fracture (Broken Bone).
-
Shenton line and angular anatomy of the femur.
-
Femoral head fractures. Top diagram is a single-fragment femoral head fracture. Bottom diagram is a comminuted femoral head fracture.
-
Femoral neck fractures. Top diagram is a nondisplaced, or incomplete, femoral neck fracture. Bottom diagram is an impacted femoral neck fracture.
-
Partially displaced femoral neck fracture.
-
Completely displaced femoral neck fracture.
-
Trochanteric fractures. Top diagram is a nondisplaced trochanteric fracture. Bottom diagram is a displaced trochanteric fracture.
-
Intertrochanteric fractures. Top diagram is a single fracture line intertrochanteric fracture. Bottom diagram is a displaced, or multiple fracture line, intertrochanteric fracture.









