Practice Essentials
Contact stomatitis describes an inflammatory reaction of the oral mucosa by contact with irritants or allergens (see the images below). Contact stomatitis is classified by its clinical features, pattern of distribution, or etiologic factors. Contact stomatitis frequently goes undetected because of the scarcity of clinical signs that are often less pronounced than subjective symptoms. [1, 2, 3]
Also see Denture Stomatitis and Nicotine Stomatitis (Smoker's Palate).

Pathophysiology
Normally, the oral mucosa is relatively resistant to irritants and allergens due to the following anatomical and physiological factors [4, 5] :
-
High vascularization that favors absorption and prevents prolonged contact with allergens
-
Low density of Langerhans cells and T lymphocytes
-
Dilution of irritants and allergens by saliva that also buffers alkaline compounds
Prognosis
The prognosis for contact stomatitis is excellent if the causative agent is detected and removed. Contact stomatitis usually resolves without sequelae.
Patient education
Teach avoidance if a causative agent is identified (see Diet).
Signs and symptoms
Acute contact stomatitis is easily correlated to the causative agent; however, contact stomatitis most frequently presents as a chronic condition. Tracing the relationship between contact stomatitis and causative factors is difficult. The presence of lip and perioral eczema aids in making the diagnosis. Symptoms of contact stomatitis include the following [4, 6] :
-
Burning sensation
-
Pain
-
Paresthesia
-
Numbness
-
Bad taste
-
Excessive salivation
-
Perioral itching
Also see Physical Examination.
Diagnostics
Serologic testing may be helpful. In vitro tests, such as a radioallergosorbent test (RAST), for specific immunoglobulin E are available for food and latex allergy. These tests can confirm sensitivity and establish the degree of allergy.
Also see Procedures and Histologic Findings.
Treatment
Removal of the causative agent is essential in contact stomatitis.
Systemic steroids are rarely required for contact stomatitis. Intraoral topical steroids are prescribed in severe cases of contact stomatitis. Topical steroids are the first-line therapy for contact stomatitis. Available vehicles include topical gels, creams, pastes, ointments, sprays, and rinses. General guidelines for administration and usage can be found in standard pharmacology references.
Sucking on ice cubes provides temporary relief from contact stomatitis.
Consultations
Consult with a dermatologist for evaluation of underlying skin disorders and for patch testing.
Consult with dentists for evaluation of dental restorations and teeth occlusion.
Etiology
Ingredients of dentifrices, mouthwashes, and dental cleaners (rare) are possible causes of irritant or allergic contact stomatitis. [7, 8, 9, 10]
Flavoring agents (eg, cinnamon compounds, eugenol, menthol) have been implicated. [11]
Colophony in dental floss and denture adhesives have also been reported causes of irritant or allergic contact stomatitis. [5, 12, 13]
Antimicrobials reportedly to have caused irritant or allergic contact stomatitis include chlorhexidine and quaternary ammonium compounds.
Ingredients of candies and chewing gums that may cause irritant or allergic contact stomatitis include flavoring agents (rare) (cinnamon compounds, menthol) and propolis, a strong sensitizer often used in the oral cavity because of its antiseptic properties.
Cosmetic ingredients (fragrance and preservatives) are a common cause of contact cheilitis. [14]
Ingredients in dental restorations may be responsible. [15, 16, 17] Amalgam fillings contain mercury compounds (45-60%) and often gold, palladium, and platinum. [18, 19, 20, 21, 22, 23, 24] Metallic and ammoniated mercury are common sensitizers. Dental cement used for sealing pulp canals may contain eugenol, balsam of Peru, and colophony. Acrylic fillings rarely cause problems in dental patients because polymerization of the resin occurs without contact between the sensitizing acrylic monomers and the oral mucosa, and the final polymerized acrylate is relatively free of allergens. [25]
Ingredients of dental prosthesis are reported to cause irritant or allergic contact stomatitis. [26, 27] Metal prostheses may release nickel, especially when they are poorly made or corroded (see the image below).
 Allergic contact stomatitis on the gingiva in a patient with a positive patch test result to nickel, palladium, and mercury.
Allergic contact stomatitis on the gingiva in a patient with a positive patch test result to nickel, palladium, and mercury.
Nickel is also present in dental braces, bridges, and crowns (see the image below). Contact gastritis due to nickel has also been reported. [28]

Stomatitis from acrylates is rare. Acrylate sensitization is a common occupational problem in dentists and dental technicians. It has been reported in 2-3% of dental patients. [29, 30, 31]
Topical drugs, such as antibiotics, anesthetics, antiseptics, and steroids, may cause sensitization. [32]
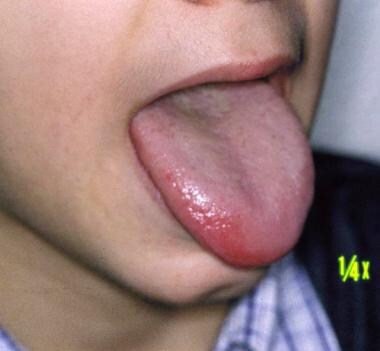
Rubber (eg, gloves, dams, orthodontic elastics, bite blocks) may cause sensitization. [33] Latex allergy is not rare (see the images below).

 Close-up view of contact urticaria of the tongue in a patient with latex allergy.
Close-up view of contact urticaria of the tongue in a patient with latex allergy.
Foods [34] rarely cause contact stomatitis. Children with atopic dermatitis and a food allergy may develop contact urticaria with lip swelling and stomatitis after contact with foods, especially fruits (eg, fruits of the Rosaceae family [eg, apple, peach, pear] in patients with birch pollinosis). Food allergy can worsen granulomatous cheilitis. Gallates in margarine and other oily foods can cause stomatitis and cheilitis. [35] Alcoholic beverages, such as sweet vermouth, [36] and propolis-containing candies [37, 38] have been reported as causing contact stomatitis.
Ingredients in cosmetics, lipsticks, lip balms [39] , and the sunscreens in these products (eg, propolis, ricinoleic acid, colophony derivatives) may cause contact stomatitis (see the images below).
 Acute allergic stomatitis involving the oral mucosa and the lip due to benzocaine.
Acute allergic stomatitis involving the oral mucosa and the lip due to benzocaine.
 Allergic contact dermatitis involving the lips and the perioral area due to propolis.
Allergic contact dermatitis involving the lips and the perioral area due to propolis.
Tobacco consumption can be responsible for nicotine stomatitis, black hairy tongue, periodontal disease, and contact stomatitis. [40, 41]
Epidemiology
Frequency
United States
The exact incidence of contact stomatitis is unknown; however, numerous well-documented series of patients with this disorder are described in the literature. Irritant reactions appear to be more common than allergic reactions.
International
In Europe, an estimated 0.01% of the population has oral symptoms related to dental materials. [42] Patch testing identifies a contact allergy in no more than 10% of these patients. Allergic reactions are usually intraoral (68%), and responsible materials are more commonly latex, metals, resins, and hygiene products. Patients with oral mucosal diseases are significantly more likely to have demonstrable hypersensitivity to food additives, especially benzoic acid, and perfumes and flavorings, especially cinnamaldehyde, compared with controls. [43]
Sex
No sexual predilection is known for contact stomatitis, except for the burning mouth syndrome that almost exclusively affects women.
Age
Contact stomatitis may occur in persons of any age, but it is much more common in elderly individuals. A study evaluating oral lesions among elderly people revealed denture-induced stomatitis in 17.2% of patients aged 65-99 years. [44] Allergic contact stomatitis to nickel seems to be more frequent in young females with a clinical history of allergies; it is not associated with how long the patients are exposed to fixed orthodontic appliances.
-
Irritant contact stomatitis of the tongue.
-
Close-up view of irritant contact stomatitis of the tongue.
-
Acute allergic stomatitis involving the oral mucosa and the lip due to benzocaine.
-
Allergic contact dermatitis involving the lips and the perioral area due to propolis.
-
Allergic contact reaction due to nickel in a dental brace.
-
Allergic contact stomatitis on the gingiva in a patient with a positive patch test result to nickel, palladium, and mercury.
-
Leukoplakialike lesion in a patient who is allergic to mercury.
-
Lichen planus–like lesion adjacent to a dental restoration.
-
Contact urticaria of the lip due to food allergy.
-
Contact urticaria of the tongue in a patient with latex allergy.
-
Close-up view of contact urticaria of the tongue in a patient with latex allergy.
-
Positive patch test result to mercury.
-
Positive prick test result to latex.




