Practice Essentials
Basal cell carcinoma (BCC) and cutaneous squamous cell carcinoma (cSCC) are the first and second most common types of skin cancer, respectively. Other significant skin lesions are actinic keratosis and melanoma. Actinic keratosis and BCC are easily excised and have a very good prognosis, while cSCC has a poor prognosis, especially if it invades the lymph nodes and adjacent vital structures. Actinic keratosis is the premalignant precursor for cSCC, and early treatment will save the patient morbidity. Extrinsic factors, such as ultraviolet light from sun exposure, are linked to cSCC, while intrinsic factors, such as the use of antioxidants, aspirin, and nonsteroidal anti-inflammatory drugs (NSAIDs), [1, 2] are reported to reduce the risk of developing the disease. [3] A biopsy should be performed for any lesion suspected of being a cutaneous neoplasm. For invasive cSCC, surgical excision and Mohs micrographic surgery are the primary treatment options. [4, 5]
Signs and symptoms of cutaneous squamous cell carcinoma
Clinically, cSCC presents as a shallow ulcer with elevated margins, often covered by a plaque and usually located in a sun-exposed area. Typical surface changes may include scaling, deep ulceration, crusting, and cutaneous horn.
A less common presentation of cSCC includes a pink cutaneous nodule without overlying surface changes. Regional metastasis of head and neck cSCC may result in enlarged and palpable submandibular or cervical lymph nodes.
If cSCC invades the adjacent peripheral nerve, it causes numbness, pain, and muscle weakness. These may be some of the clinical signs of invasion other than palpable lymph nodes.
Diagnosis of cutaneous squamous cell carcinoma
Diagnostic workup of suspected cSCC will include computed tomography (CT) scanning to evaluate for soft tissue or bony invasion and lymph node metastasis. Magnetic resonance imaging (MRI) may be used to rule out invasion of neural or vital structures. Incisional or excisional biopsy are essential for definitive diagnosis. The choice of biopsy will depend on the size and location of the lesion.
Management of cutaneous squamous cell carcinoma
Treatment options include the following:
-
Surgical excision with clear margins, as verified by frozen sections
-
Mohs micrographic surgery for invasive cSCC in the facial region
-
Radiation therapy as an adjuvant to surgery, to provide improved locoregional control, or as primary therapy in patients who are unable to undergo surgical excision
-
Chemotherapy, such as treatment with oral 5-fluorouracil (5-FU) and epidermal growth factor receptor (EGFR) inhibitors, as adjuvant therapy for select highest-risk cases
-
Systemic chemotherapy for metastatic cSCC
Background
Cutaneous squamous cell carcinoma (cSCC) is the second most common skin cancer and one of the most common cancers overall in the United States. [3]
Despite increased knowledge and public education regarding the causes of skin cancer and modes of prevention, the incidence of cSCC continues to rise worldwide. This increasing incidence is likely multifactorial; the speculated causes for the rise include an aging population, improved detection, an increased use of tanning beds, and environmental factors, such as depletion of the ozone layer.
Although cSCC is not often fatal, it can cause significant morbidity, especially when it involves the facial skin. Most cSCCs are located in the head-and-neck region, and extensive excision required in an advanced stage of the disease can cause disfigurement. Furthermore, the cost of treatment has been shown to pose a significant public health burden. In a study of the US Medicare population, the treatment of nonmelanoma skin cancers ranked fifth among the most expensive cancers to treat in the head-and-neck region.
Diagnosis of cSCC begins with a careful history and physical examination. A biopsy should be performed for any lesion suspected of being a cutaneous neoplasm to rule out basal cell carcinoma and other dermal lesions.
Given the central role that ultraviolet radiation (UVR) plays in the pathogenesis of cSCC, methods aimed at decreasing UVR exposure form the cornerstone of cSCC prevention. In addition, treatment of precancerous lesions and in situ SCC may prevent the future development of invasive lesions.
Chemotherapy may be considered as adjuvant therapy in select highest-risk cases of cSCC. In particular, emerging evidence suggests that epidermal growth factor receptor (EGFR) inhibitors may be useful adjuncts to surgical treatment. Systemic chemotherapy may be considered for metastatic cSCC.
By convention, the term head-and-neck SCC typically refers to SCC of the mucosal linings of the oral cavity and upper respiratory tract, while cSCC involves the skin.
Pathophysiology
Malignant transformation of normal epidermal keratinocytes is the hallmark of cSCC. One critical pathogenic event is the development of apoptotic resistance through functional loss of TP53, a well-studied tumor suppressor gene. TP53 mutations are seen in over 90% of skin cancers diagnosed in the United States, as well as in most precursor skin lesions, suggesting that loss of TP53 is an early event in the development of cSCC. [6]
UVR causes deoxyribonucleic acid (DNA) damage through the creation of pyrimidine dimers, a process known to result in the genetic mutation of TP53. Upon subsequent UVR exposure, keratinocytes undergo clonal expansion, acquiring further genetic defects, ultimately leading to invasive cSCC.
Many other genetic abnormalities are believed to contribute to the pathogenesis of cSCC, including mutations of BCL2 and RAS. Likewise, alterations in intracellular signal transduction pathways, including the epidermal growth factor receptor (EGFR) and cyclo-oxygenase (COX), have been shown to play a role in the development of cSCC.
Squamous cell carcinoma in situ (CIS), sometimes referred to as Bowen disease, is a precursor to invasive cSCC. Characteristics of this lesion include nuclear atypia, frequent mitoses, cellular pleomorphism, and dyskeratosis, parakeratosis, and hyperkeratosis.
CIS is differentiated from actinic keratosis, a similar precancerous skin lesion, by the full-thickness involvement of the epidermis in CIS. Invasive cSCC is differentiated from CIS and actinic keratosis by the invasion of the basement membrane by malignant-appearing cells. With invasive cSCC, nests of atypical cells are found within the dermis, surrounded by an inflammatory infiltrate.
Conventional cSCC can be divided into the following four histologic grades, based the degree of nuclear atypia and keratinization found (see the image below):
-
Well differentiated - Characterized by more normal-appearing nuclei with abundant cytoplasm and extracellular keratin pearls
-
Moderately differentiated - Exhibits features intermediate between well-differentiated and poorly differentiated lesions
-
Poorly differentiated - Shows a high degree of nuclear atypia with frequent mitoses, a greater nuclear-cytoplasmic ratio, and less keratinization
-
Highly undifferentiated - Shows epithelial cells that may be difficult to distinguish from mesenchymal, melanoma, or lymphoma cells
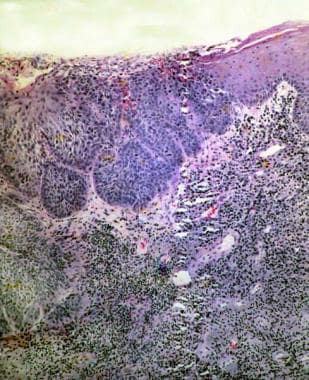 Squamous cell carcinoma. The lesion closely approximates the specimen in the previous image. Field cancerization is illustrated; that is, if >1 cell is exposed to a carcinogen, >1 cell becomes cancerous. Note the marked inflammatory-cell response. Should limited biopsy reveal only severe atypia with a severe inflammatory response, the lesion should be investigated further, because a cancer is likely nearby.
Squamous cell carcinoma. The lesion closely approximates the specimen in the previous image. Field cancerization is illustrated; that is, if >1 cell is exposed to a carcinogen, >1 cell becomes cancerous. Note the marked inflammatory-cell response. Should limited biopsy reveal only severe atypia with a severe inflammatory response, the lesion should be investigated further, because a cancer is likely nearby.

Other histologic variants include acantholytic (adenoid) SCC, which is characterized by a pseudoglandular appearance, and spindle cell SCC, which has atypical, spindle-shaped cells. Both of these variants exhibit a more aggressive clinical course.
Etiology
Exposure to cancer-promoting stressors and the response of the body to those exposures (host response) promote the development of cSCC. Well-known risk factors include the following:
-
UVR exposure
-
Immunosuppression
-
Exposure to ionizing radiation or chemical carcinogens
-
Human papillomavirus (HPV) infection
Chronic UVR exposure, such as through tanning beds, medical UV treatments, or cumulative lifetime sun exposure, is the most important risk factor for the development of cSCC. UVR is a known mutagen capable of inducing DNA damage that can lead to keratinocyte transformation. UVR has also been shown to alter the cutaneous immune response, leaving the skin susceptible to tumor formation. [7]
A number of surrogate indices of chronic UVR exposure from the sun are well known. Specifically, epidemiologic evidence suggests that geographic proximity to the equator, a history of precancerous lesions or prior skin cancers, older age, and male sex predispose an individual to the development of cSCC.
Immunosuppression is also increasingly recognized as a risk factor for the development of skin cancer; this is true of iatrogenic and noniatrogenic immunosuppression (eg, in organ transplant recipients and persons with the human immunodeficiency virus (HIV), respectively). Regardless of the reason for immunosuppression, cSCC that arises in the setting of immunosuppression exhibits a more aggressive course, with a higher rate of local recurrence, metastasis, and death.
Host responses that influence cSCC development include genetic predisposition to DNA damage and, in particular, susceptibility to UVR damage. Well-known markers for UVR vulnerability include the following:
-
Fair skin (or a history of repeated sun exposure)
-
Albinism
A rare genetic defect that affects the repair mechanism for UVR-induced DNA damage, resulting in xeroderma pigmentosum, has been causally linked to UVR-induced cSCC. Xeroderma pigmentosum is characterized by severe sensitivity to UVR and premature development of cSCC.
A genetic study by Schwaerderle et al using next-generation sequencing indicated that seven genes (TP53, PIK3CA, CCND1, CDKN2A, SOX2, NOTCH 1, FBXW7) are altered more frequently in various types of SCC (including cSCC) than in non-SCC, while an eighth gene, KRAS, is altered less frequently in SCC. [8]
Dermatoses that influence or enhance cSCC development include the following:
-
Xeroderma pigmentosum
-
Dystrophic epidermolysis bullosa
-
Epidermodysplasia verruciformis
A retrospective study by Ahadiat et al suggested that an association exists between hypothyroidism and the development of cSCC, with the rate of cSCC patients in the study who had a preceding diagnosis of hypothyroidism (23%) being significantly higher than the rate of people in the general population with hypothyroidism. [9]
A study by Pedersen et al indicated that hydrochlorothiazide (HCTZ), one of the most frequently prescribed diuretic and antihypertensive drugs in the United States and Western Europe, raises the risk for BCC and cSCC. HCTZ has a photosensitizing effect and, in an experimental model, was seen to encourage UVA-induced DNA damage. The investigators reported an association between a high amount of HCTZ use (50,000 mg or more) and odds ratios for BCC and cSCC of 1.29 and 3.98, respectively. The odds ratios rose to 1.54 and 7.38, respectively, for patients with a cumulative HCTZ dose of 200,000 mg or more. [10, 11]
UVR exposure
The component of sunlight believed to be most important in cutaneous carcinogenesis is UVB (290-320 nm), which is an initiator and a promoter of carcinogenesis. In animal models, UV-induced photocarcinogenesis appears to involve the UVB and UVA-2 spectral ranges. [12]
UV-light treatments used for psoriasis (and other recalcitrant dermatoses) also predispose to the development of SCC. Psoralen and UVA (PUVA) therapy is particularly phototoxic, with mutations in both TP53 and the oncogene Ha -Ras being present in a large proportion of patients with PUVA-associated cSCC. [13] In addition to being mutagenic, UVA in conjunction with UVB is a potent suppressor of the cutaneous immune system, which likely contributes to its role in cutaneous carcinogenesis.
Fair complexion
Persons with a fair complexion; hazel, blue, or gray eyes; and light-colored hair (blond or red), as well as those who burn easily when exposed to the sun, are at higher risk for cSCC than are persons with other physical characteristics. Individuals with Fitzpatrick skin types I and II account for most of the patients who develop SCC.
Patients with oculocutaneous albinism are also at risk; SCCs account for the most common type of cutaneous malignancy in this group. Such individuals lack natural protection from UV-induced carcinogenesis, owing to reduced levels of the photoprotective pigment, melanin. [14]
DNA repair failure
Healthy human skin is constantly repairing UV-induced damage through DNA repair mechanisms. Patients with xeroderma pigmentosum have a deficiency in an enzyme essential for normal DNA repair and are thus prone to the development of innumerable SCCs and, less commonly, other cutaneous tumors. [15]
Immunosuppression
The specific mechanisms by which immunosuppression leads to SCC development are poorly understood, but diminished immunosurveillance is thought to be critical. CD8+ T cells specific for the tumor suppressor gene TP53 have been observed in patients with SCC, suggesting that a functional immune system may target keratinocytes expressing mutated TP53. [16] Suppression of the immune system would presumably abrogate this response, possibly facilitating the development of SCC.
Iatrogenic immunosuppression
For organ transplant recipients on long-term immunosuppressive treatment, skin cancers account for 90% of all diagnosed malignancies. [17] In this group of patients, cSCC is more common than other keratinocyte-derived neoplasms, including BCC.
The use of immunosuppressive medications to prevent rejection in organ transplant recipients is associated with a 65- to 250-fold increased risk of developing SCC compared with the general population. [18] Additionally, organ transplant recipients have a high risk of developing further SCCs, with 66% developing a second SCC within 5 years of their first SCC diagnosis. [19]
The degree of risk correlates with the intensity of immunosuppression (ie, number and/or dosage of medications) typically required to prevent rejection in this patient population. For example, heart transplant recipients have 3 times the risk of SCC compared with kidney transplant recipients.
However, while the proportion of recipients developing new tumors is greater with heart transplants than with kidney transplants, the mean number of tumors per patient is higher in kidney transplant recipients. This may be due to a longer duration of immunosuppression in kidney transplant patients, who tend to be younger than patients who undergo heart transplantation. [19]
The primary risk factor in organ transplant patients is cumulative lifetime UV exposure in combination with having Fitzpatrick skin type I or II. The risk of SCC also increases with the number of years post-transplantation, presumably because of the cumulative effects of prolonged immunosuppressive therapy.
Not only is SCC a more frequent occurrence in organ transplant recipients, the tumors can be very aggressive clinically. In a study of cardiothoracic transplant recipients (heart or heart-lung transplants), 4% of patients developed aggressive cSCC within 10 years of transplantation. [20] The majority (15 of 18) of the lesions were poorly differentiated, and two thirds of the patients with aggressive lesions had distant-organ metastases or died of their disease.
Pretransplantation end-organ disease may also impact the development of post-transplant SCC. For example, among renal transplant recipients, the highest prevalence of skin cancer was observed in patients with polycystic kidney disease, whereas the lowest incidence was seen in those with diabetic nephropathy. Similarly, cholestatic liver disease was associated with a greater post-transplantation risk of skin cancer compared with other causes of liver failure.
Noniatrogenic immunosuppression
Patients with HIV-associated immunosuppression have a more modestly elevated risk of developing a nonmelanoma skin cancer (3-5 times that of the general population). However, they do not have the altered SCC-to-BCC ratio typical of transplant recipients. [21]
Defects in cell-mediated immunity related to lymphoproliferative disorders (eg, chronic lymphocytic leukemia) predispose to the development of aggressive SCC.
Epidemiology
Skin cancers are the most frequently diagnosed cancers in the United States. Determining the number of cSCCs is difficult, however, because reporting of these cases to cancer registries is not required. One report estimated that in 2012, the most recent date for which these figures have been determined, there were over 5.4 million nonmelanoma skin cancers in the United States, with more than 3.3 million people treated. [22] In comparison, the American Cancer Society estimated that 2,001,140 new cases of cancer other than BCC and SCC would be diagnosed in 2024. (Cases of carcinoma in situ located at any site except the urinary bladder were also not included in the figure.) [23]
Of nonmelanoma skin cancers, approximately 80% are basal cell carcinoma (BCC) and 20% are squamous cell carcinoma (SCC). Thus, cSCC is the second most common skin cancer and one of the most common cancers overall in the United States.
Rising incidence
Despite increased knowledge and public education regarding the causes of skin cancer and the importance of avoiding prolonged sun exposure, the incidence of cSCC continues to rise worldwide. A study from South Korea looking at skin cancer incidences between 1999 and 2014 found that the incidence of SCC in that country rose steadily in those years, with the average annual percentage change in men and women being 3.3 and 6.8, respectively. [24] In Rochester, Minnesota, the annual age-adjusted incidence rates for SCC per 100,000 women rose from 47 cases from 1984-1986 to 100 cases from 1990-1992; the corresponding rates for men increased from 126 cases to 191 cases per 100,000 population. [25]
Looking at the incidence of cSCC and melanoma in seven mid- to high-latitude populations, specifically those of Finland, Norway, Sweden, Denmark, Scotland, the Netherlands, and Tasmania (Australia), Olsen et al found that between 1989 and 2020 (1989-2018 for Tasmania), the ratio of the incidence of cSCC to melanoma grew. By the most recent time period studied, cSCC had a higher incidence than melanoma did in all seven populations. [26]
The international rise in the incidence of cSCC is likely multifactorial; speculated causes include an aging population, improved detection, increased use of tanning beds, and environmental factors, such as depletion of the ozone layer.
Additionally, the number of patients on immunosuppressive therapy, used in solid organ transplantation and various rheumatologic and dermatologic conditions, is increasing. As noted previously, solid organ transplant recipients have a markedly elevated risk of SCC formation. Metastasis may also be more common in this group.
Geography-related demographics
Patients who live in greater proximity to the equator tend to present with cSCC at a younger age than do patients who live more distant from it.
In the aforementioned study by Olsen and colleagues, which looked at the populations of Finland, Norway, Sweden, Denmark, Scotland, the Netherlands, and Tasmania (Australia), the investigators found that the ratio of the incidence of cSCC to melanoma increased the closer a population was to the equator. [26]
The highest incidence of cSCC occurs in Australia, where nonmelanoma skin cancer incidences as high as 1.17 per 100, a rate 5 times greater than all other cancers combined, have been reported. [27] The high incidence is likely due to the large numbers of light-skinned people in this region who have had extensive sun exposure. [28]
Race-related demographics
SCC is the second leading cause of skin cancer in white individuals. Persons of Irish or Scottish ancestry have the highest prevalence in the United States. SCC is relatively uncommon in people of African or Asian descent. However, SCC in black persons carries a higher mortality rate, perhaps due to delayed diagnosis, because tumors are more likely to occur in sun-protected areas in these individuals, including the scalp and sites of previous injury and scarring. [29]
Sex- and age-related demographics
SCC occurs in men 2-3 times more frequently than it does in women, most likely as a result of higher cumulative lifetime UV exposure in men. This increased exposure may be due to greater participation by men in occupations that entail more significant exposure to sunlight or to other occupational hazards, such as soot, oils, or tars.
In the previously described study by Olsen et al, which examined the populations of Finland, Norway, Sweden, Denmark, Scotland, the Netherlands, and Tasmania (Australia), males had a higher incidence ratio for cSCC to melanoma than women did, but in most of the populations, women demonstrated a greater increase in the ratio over time. This suggests, according to the investigators, that UVR exposure in women has increased. [26]
The typical age at presentation for SCC is approximately 70 years. This varies widely, however, and in certain high-risk groups (eg, organ transplant recipients, patients with epidermolysis bullosa), SCC often manifests at a much younger age.
Prognosis
Although primary cSCC is not often fatal, it can cause significant morbidity if left untreated. Most cSCCs are located in the facial and head-and-neck region, where surgery for advanced-stage disease can be disfiguring.
Furthermore, the cost of treatment has been shown to pose a significant public health burden. In a study of the Medicare population, the treatment of nonmelanoma skin cancers ranked fifth among the most expensive cancers to treat. [30]
Like many cancers, cSCC is staged clinically by tumor and node size and metastasis, ie, the TNM staging system, as devised by the American Joint Committee on Cancer (AJCC). [31]
Although TNM staging is useful for estimating the outcome for a group of patients with cSCC who have similar tumor characteristics, it cannot estimate the risk for an individual patient. Current methods for estimating the outcome of a patient with cSCC depend heavily on the total excision of the lesion, with clear margins verified by frozen sections.
Despite the inherent limitations of TNM staging, the outcomes of patients with cSCC follow a predictable pattern. Most patients present with early stage tumors, and most of these patients fare well (overall 5-yr survival rate >90%) when the tumors are adequately treated.
The outcome of patients with advanced-stage cSCC is considerably worse. For patients with lymph node metastases, the 5-year survival rate is even lower, estimated at 25-45%. Tumor-related factors such as location, diameter, depth, and cellular differentiation determine the rate of recurrence, as well as perineural invasion and distant metastasis.
Diameter and thickness
Lesions of invasive SCC measuring smaller than 2 cm in diameter have been associated with a 9.1% rate of metastasis, whereas those larger than 2 cm in diameter have a metastatic rate of up to 30.3%. A prospective study reported a 3-year, disease-specific survival rate of 67% for lesions larger than 4 cm, compared with 93% for tumors smaller than 4 cm. [32]
A study by Eigentler et al indicated that in cases of cSCC, factors contributing to a high risk for tumor-specific death, if a cut-off for tumor thickness of 6 mm or greater is used, include desmoplastic growth and immunosuppression. [33]
Depth
With increasing depth of invasion of the primary SCC tumor, the risk of local recurrence and nodal metastasis increases and the rate of survival decreases. Lesions with a depth of less than 2 mm rarely metastasize; those with a depth of invasion of 2-4 mm have a historical recurrence rate of 5.3% and a metastasis rate of 6.7%.
Cellular differentiation
More poorly differentiated tumors have a worse prognosis in SCC, with reported recurrence rates of 33-54%. [34] The actual value of histologic grading alone, however, is less clear, because poorly differentiated tumors that metastasize or recur usually have additional primary risk factors (eg, large diameter, greater depth). Nonetheless, poorly differentiated lesions are generally considered to behave more aggressively.
Tumor recurrence
Recurrence risk is increased with high-risk tumors; lesions larger than 2 cm recur at a rate of 15.7% after excision. Poorly differentiated lesions recur at a rate of 25% after excision, as opposed to well-differentiated lesions, which recur at a rate of 11.8%.
Local recurrence rates following extirpation of a recurrent SCC range from 10% to 23%. Reported rates of metastasis are as high as 25-45%, but these figures may overestimate the risk in recurrences that are caught early.
Perineural invasion
Perineural invasion has been estimated to occur in up to 14% of persons with cutaneous SCC. The prognosis in such cases is worse, with historical rates of metastasis reported to be as high as 47%. Much lower rates of metastasis (8%) have been reported using Mohs micrographic surgery. [34] The degree of nerve involvement likely has a large impact on prognosis.
Involvement of major (ie, named) nerve branches carries a very high risk of recurrence. The risks are substantially decreased when tumor-free margins are painstakingly obtained by removal of the involved nerve. However, the prognosis is still guarded.
One study showed the diameter of involved nerves to significantly impact outcomes in cSCC. No disease-specific deaths occurred in patients with involvement of nerves that were less than 0.1 mm in diameter, compared with 32% of patients dying from cSCC when nerves of 0.1 mm or larger were involved. [35]
Lymph node ratio
A study by Vasan et al indicated that in patients with metastatic head and neck cSCC, a ratio of positive lymph nodes to resected lymph nodes of over 6% is a risk factor for shorter disease-free and overall survival. [36]
Patient Education
Patients with precancerous lesions should be counseled to avoid excessive UVR by limiting outdoor activity to early morning and late afternoon, using protective clothing, and wearing a broad-brimmed hat to shade the face, head, and neck. Daily application of a broad-spectrum sunscreen with a sun protection factor (SPF) of at least 15 should also be encouraged. The use of artificial tanning devices should be strongly discouraged because this has been associated with a 2.5-fold increase in the risk of developing cSCC.
Lesions can recur even years after excision, so patients should have routine examinations. In addition, patients should be counseled regarding treatment of areas of chronic skin inflammation or trauma to prevent the future development of cSCC at those sites.
Educating people who live in tropical areas and in regions with a high degree of solar exposure is particularly important.
These measures are also critically important for patients who are immunosuppressed, and they should be an integral part of the educational program for patients who have recently undergone organ transplantation.
-
Large, sun-induced squamous cell carcinoma (SCC) on the forehead/temple. Image courtesy of Glenn Goldman, MD.
-
Preauricular and helical scars (black arrows) from prior excisions are noted in a patient who presented with cervical metastases (white arrow) from an occult cutaneous squamous cell carcinoma.
-
Contrast-enhanced, axial computed tomography (CT) scan of a patient with soft tissue invasion of the right parotid gland (arrow) by an ulcerative cutaneous squamous cell carcinoma.
-
Large, neglected cutaneous squamous cell carcinoma of the right ear that requires wide local excision via auriculectomy and reconstruction. The risk of lymph node metastasis with this deeply ulcerative tumor is high enough to warrant elective neck dissection.
-
Squamous cell carcinoma in situ (Bowen disease). Courtesy of Hon Pak, MD.
-
Extensive conjunctival squamous cell carcinoma of the left eye. The patient had limbal and corneal involvement temporally, as well as scleral invasion with intraocular spread. A malignant cellular reaction in the anterior chamber was present. The patient was treated with a lid-sparing exenteration.
-
A 35-year-old man with human immunodeficiency virus (HIV) infection presented with a 2-year history of a slowly enlarging, left lower eyelid lesion; incisional biopsy revealed squamous cell carcinoma.
-
Axial magnetic resonance image (MRI) of a large squamous cell carcinoma of the left lower eyelid with invasion of the anterior orbit.
-
A large, ulcerated, invasive squamous cell carcinoma of the left lower eyelid. This patient also had perineural invasion of the infraorbital nerve extending into the cranial base.
-
Progressively severe atypia. The epithelium to the left is close to normal, but the epithelium to the right shows full-thickness atypia (ie, carcinoma in situ). This image illustrates carcinogenesis, the process whereby cells exposed to a carcinogen become cancerous over time.
-
Squamous cell carcinoma. The lesion closely approximates the specimen in the previous image. Field cancerization is illustrated; that is, if >1 cell is exposed to a carcinogen, >1 cell becomes cancerous. Note the marked inflammatory-cell response. Should limited biopsy reveal only severe atypia with a severe inflammatory response, the lesion should be investigated further, because a cancer is likely nearby.
Tables
Stage |
Primary Tumor |
Regional Lymph Nodes |
Distant Metastasis |
Stage 0 |
Tis |
N0 |
M0 |
Stage I |
T1 |
N0 |
M0 |
Stage II |
T2 |
N0 |
M0 |
Stage III |
T3 |
N0 |
M0 |
T1-3 |
N1 |
M0 |
|
Stage IV |
T4 |
N0 |
M0 |
Any T |
N2-3 |
M0 |
|
Any T |
Any N |
M1 |






